Drop the steak knife. After a controversial study last fall recommending that it was not necessary for people to change their diet in terms of red meat and processed meat, a large, carefully analyzed new study links red and processed meat consumption with slightly higher risk of heart disease and death, according to a new study from Northwestern Medicine and Cornell University.
Eating two servings of red meat, processed meat or poultry—but not fish—per week was linked to a 3 to 7% higher risk of cardiovascular disease, the study found. Eating two servings of red meat or processed meat—but not poultry or fish—per week was associated with a 3% higher risk of all causes of death.
“It’s a small difference, but it’s worth trying to reduce red meat and processed meat like pepperoni, bologna and deli meats,” said senior study author Norrina Allen, associate professor of preventive medicine at Northwestern University Feinberg School of Medicine. “Red meat consumption also is consistently linked to other health problems like cancer.”
“Modifying intake of these animal protein foods may be an important strategy to help reduce the risk of cardiovascular disease and premature death at a population level,” said lead study author Victor Zhong, assistant professor of nutritional sciences at Cornell, who did the research when he was a postdoctoral fellow in Allen’s lab.
The paper will be published Feb. 3 in JAMA Internal Medicine.
The new findings come on the heels of a controversial meta-analysis published last November that recommended people not reduce the amount of red meat and processed meat they eat. “Everyone interpreted that it was OK to eat red meat, but I don’t think that is what the science supports,” Allen said.
“Our study shows the link to cardiovascular disease and mortality was robust,” Zhong said.
What should we eat?
“Fish, seafood and plant-based sources of protein such as nuts and legumes, including beans and peas, are excellent alternatives to meat and are under-consumed in the U.S.,” said study coauthor Linda Van Horn, professor of preventive medicine at Feinberg who also is a member of the 2020 U.S. Dietary Guidelines Advisory committee.
The study found a positive association between poultry intake and cardiovascular disease, but the evidence so far isn’t sufficient to make a clear recommendation about poultry intake, Zhong said. Still, fried chicken is not recommended.
The new study pooled together a large diverse sample from six cohorts, included long follow-up data up to three decades, harmonized diet data to reduce heterogeneity, adjusted a comprehensive set of confounders and conducted multiple sensitivity analyses. The study included 29,682 participants (mean age of 53.7 years at baseline, 44.4% men and 30.7% non-white). Diet data were self-reported by participants, who were asked a long list of what they ate for the previous year or month.
Key findings:
A 3 to 7% higher risk of cardiovascular disease and premature death for people who ate red meat and processed meat two servings a week.
A 4% higher risk of cardiovascular disease for people who ate two servings per week of poultry, but the evidence so far is not sufficient to make a clear recommendation about poultry intake. And the relationship may be related to the method of cooking the chicken and consumption of the skin rather than the chicken meat itself.
No association between eating fish and cardiovascular disease or mortality.
Limitations of the study are participants’ dietary intake was assessed once, and dietary behaviors may have changed over time. In addition, cooking methods were not considered. Fried chicken, especially deep fat-fried sources that contribute trans-fatty acids, and fried fish intake have been positively linked to chronic diseases, Zhong said.
https://moreliaclinic.com/wp-content/uploads/2015/08/FINAL-MORELIA-LOGO1.png00adminhttps://moreliaclinic.com/wp-content/uploads/2015/08/FINAL-MORELIA-LOGO1.pngadmin2020-02-03 20:38:322020-02-03 20:38:35Eating red meat and processed meat hikes heart disease, death risk: study
Officials in China are racing to contain a deadly new strain of virus that has infected more than 2,700 people and left at least 81 dead. Chinese officials have blocked all transportation in and out of the city of Wuhan and surrounding areas, where the outbreak of the “2019 novel coronavirus” or “2019-nCoV” originated.
Five cases of the illness have been confirmed in the United States — all in people who had recently traveled from Wuhan, China. U.S. health officials confirmed the first case on Tuesday, involving a man in his 30s in Seattle. The second case was confirmed Friday in a woman in her 60s in Chicago. Health officials said she was “doing well.” Over the weekend, two additional cases were confirmed in California and one in Arizona.
The U.S. Centers for Disease Control and Prevention said Friday that more than 60 people in 22 states were being monitored for possible infection.
China locks down cities in unprecedented effort to contain coronavirus
Health officials believe the virus was initially transmitted from animals to humans, but that human-to-human transmission of the flu-like illness is now occurring.
What is a coronavirus?
Coronaviruses are a large group of viruses that can cause illnesses as minor as a cold, or as serious as Middle East Respiratory Syndrome (MERS) and Severe Acute Respiratory Syndrome (SARS), according to the World Health Organization. They often present with pneumonia-like symptoms.
The viruses can be transmitted from animals to humans; the virus that causes SARS, for example, was originally transmitted to humans from a cat-like animal called a civet. But in some instances, as appears to be the case with this new strain of coronavirus, they can also be transmitted between humans.
The World Health Organization said there are multiple known coronaviruses circulating in animals that have not yet been transmitted to humans.
How did the new strain start?
The outbreak began in Wuhan, a city of 11 million people. Many of the early patients were reportedly linked to Hua Nan Seafood Wholesale Market, a large seafood and animal market in the city, according to CBS News’ Ramy Inocencio. But since then, a rising number of people have apparently contracted the virus without exposure to the market.
The market was closed on January 1, 2020 for “environmental sanitation and disinfection,” according to the World Health Organization.
How many people have died?
At least 81 people have died from the illness, according to Chinese officials. Most of those deaths occurred in Wuhan, which is in the central Hubei province. The first death was reported January 9.
Where is it?
While the virus originated around Wuhan, cases have also been reported in Thailand, Taiwan, Japan, South Korea, Vietnam, Malaysia, Nepal, Singapore, the U.S., Australia and France.
How is it transmitted?
It’s well-established that coronaviruses can spread from animals to humans, according to the World Health Organization. But health officials confirmed there have been cases in which this virus has spread from human to human.
Chinese state-run media quoted Zhong Nanshan, a scientist at the China’s National Health Commission, as saying such transmission was “affirmative.” The scientist did not say how many cases were the result of human-to-human transmission — but in one case, a hospital patient is said to have infected 14 medical workers, reports Inocencio.
What’s being done to stop the spread?
The World Health Organization convened an emergency committee on the virus in Geneva, Switzerland. It said Thursday that the outbreak does not rise to the level of being designated an international public health emergency, but WHO will continue working with nations to contain it.
Meanwhile in the U.S., the CDC deployed public health workers to screen passengers arriving from Wuhan at five major ports of airline entry: New York-JFK, Los Angeles, San Francisco, Atlanta and Chicago-O’Hare.
The CDC said it has developed a test to diagnose the virus. Currently, that test must be administered at the CDC, but the organization is working to share the test with domestic and international partners.
In Hong Kong, which was ravaged by SARS in 2002 and 2003, hospitals upped their alert level to “serious” and implemented temperature checkpoints for inbound travelers.
While China has closed transportation in and out of Wuhan and 12 other cities, there are concerns that as hundreds of millions of people travel around the country to celebrate the Chinese New Year, the virus could spread even faster.
https://moreliaclinic.com/wp-content/uploads/2015/08/FINAL-MORELIA-LOGO1.png00adminhttps://moreliaclinic.com/wp-content/uploads/2015/08/FINAL-MORELIA-LOGO1.pngadmin2020-01-27 19:52:062020-01-27 19:52:09What is the coronavirus illness blamed for multiple deaths in China?
“I feel like I’m being poisoned.” I will never forget the night I told my parents that I thought my breast implants were the cause of a decade’s worth of unexplained medical phenomena.
What started as a sudden onset of panic attacks 7 years ago transformed into a laundry list of debilitating mental and physical ailments that I was forced to cope with daily.
The day before my explant surgery, I tallied 49 symptoms that I was actively experiencing. I had received misdiagnoses of mental health conditions, such as panic disorder, anxiety disorder, depression, PTSD, and most recently, bipolar disorder.
I struggled with bouts of extreme insomnia, where I wouldn’t sleep at all for 2 to 3 days on end.
Doctors had prescribed pretty much every combination of SSRIs, benzos, stimulants, and sleep medications on the market. The slew of debilitating side effects from these drugs landed me in the ER too many times to count.
Physically, I experienced an onset of sudden food intolerances and allergies that caused digestive issues, such as acid reflux, GERD, and gastritis.
I lived with symptoms of autoimmune diseases, such as joint pain, swollen lymph nodes, and liver and kidney dysfunction, all with no conclusive diagnosis.
My feet and hands turned purple and were ice cold to the touch. My hair fell out in clumps in the shower, and the strands that remained were dry and brittle. My blood tests showed abnormal liver and kidney function, and my kidney grew a mass twice the size of itself. I experienced other unexplained symptoms, such as skin rashes, migraines, brain fog, and numbness and tingling in extremities.
The surgery changed everything
My entire life suffered from the toxic blow of this unexplained condition. Before I got sick, I was a college senior at USC, on the Dean’s list, with an abundance of friends. I was in a healthy relationship and involved in every extracurricular activity I could fit into my overpacked schedule.
I was headed to Nashville upon graduation to pursue my dream job of working in the entertainment industry. I was free of mental and physical ailments. It was the last time I can remember being effortlessly happy. I continually asked myself, “What happened to my old life? Will I ever get it back?”
From the outside looking in, it’s hard to understand. From the inside looking out, it’s hard to explain.
It’s difficult to put into words the dichotomy my life had become because, on the outside, I looked fine, but inside, my body was waging war on itself. The truth is that this illness took everything from me that I once recognized, admired, and valued about myself. My life bore no resemblance to the version I left behind almost a decade ago.
I spent entire days stuck in bed, ruminating on to-do lists I didn’t have the energy or motivation to begin, let alone complete. I got so anxious at times that I wanted to crawl out of my skin. Each day I woke up with the hope that today would be the beginning of a new start. I put in what felt like 150% effort, while I watched others coast along.
I went to bed every night with the notion that I hadn’t achieved nearly enough. I chalked it up to another day inside a body that wouldn’t work and a mind that couldn’t stop ruminating on the pain.
I fight for my health every day in a way most people don’t understand. I’m not lazy; I am a warrior.
At the height of my illness, I was taking five prescription medications to manage the mental symptoms alone. I was taking meds to wake up, meds to concentrate, meds to relax, and meds to fall asleep.
My entire life was chemically induced, and none of my emotions felt like my own. I was also a regular in the emergency room, thanks to the physical symptoms that accompanied this illness.
Most recently, I was brought in for stroke symptoms and unexplained bleeding from my mouth. After hours of bloodwork and imaging, I was sent home with a generic, temporary Band-Aid in the form of steroids, Benadryl, and a prescription for Xanax, but no answers.
From rock bottom came the answers
I am learning to be thankful for my rock bottom, as it was the catalyst that brought me the answers I was seeking.
I went home that night, and at an all-time low, I put out a desperate Facebook post explaining my situation. I was met with a reply from a college friend, directing me to Breast Implant Illness and Healing by Nicole.
After hours of scrolling through tens of thousands of women’s stories that sounded all too familiar to me, I reached a verdict. I was sure that my breast implants were the culprit.
“Save yourself a surgery,” the plastic surgeon who fitted my implants told me when I enquired about having my 7-year-old Mentor-brand, textured, silicone breast implants removed.
“I have been in practice for over 30 years, and you are the first person who has ever wanted them taken out. You aren’t going to like the way you look without them, and you will want them put back in.”
“I strongly believe that the proper removal of my breast implants was key to my recovery.”
I still have regrets about that day. After weeks of self-conducted research, I regret not bringing him the facts I had uncovered about certain implants. Some silicone breast implants contain carcinogens, neurotoxins, and cleaning agents, among other things.
Now, I don’t claim to have an MD, but it’s hard to believe that the almost identical symptoms that myself and thousands of other women with breast implants experienced were merely a coincidence.
There is a growing body of research suggesting that breast implants can cause autoimmune disorders in some women. The Food and Drug Administration (FDA) released a worldwide recall of Allergan textured breast implants last month in a bid “to protect women from breast implant-associated anaplastic large cell lymphoma.”
If you have breast implants, don’t panic. First, focus on identification of your symptoms and then move to explant.
I strongly believe that the proper removal of my breast implants was key to my recovery. An international list of recommended explant surgeons can be found here.
The detoxification process can take up to 2 years, so even though I have removed the source of my suffering, the symptoms still come and go like a clingy house guest who doesn’t pick up on social cues.
Recovery and rediscovering myself
I am now 2 months post-op and am already seeing improvements. Before my surgery, I had bloodwork done, and my liver enzymes were indicative of someone with lifelong alcohol dependency. Recently, my bloodwork has miraculously normalized.
The symptoms seem to be falling away one by one. The physical symptoms I mentioned, such as skin rashes, stroke symptoms, flu symptoms, and liver and kidney issues, have all gone. I have lost 30 pounds already, all of which was inflammation weight. I have even started weening myself off of antidepressants, as I feel so much stronger mentally.
For the first time in a decade, when I look in the mirror, I recognize the person staring back at me. We all have the same hours in a day, and this illness has taught me how to live them with purpose, to treasure every alert moment, and relish every second of pain free bliss. My perspective is shifting from hopeless to limitless.
The best part about recovery is when we get to rediscover ourselves, to find our passion, and to find our purpose.
I am still learning how to be thankful for my struggle because, without it, I wouldn’t have stumbled across my strength. I am learning that I’m not a victim for sharing my story, but a survivor setting the world on fire with my truth.
I am no longer ashamed of my journey, as I have emerged with an appreciation, a sensitivity, and an understanding of life that fills me with compassion, gentleness, and a deep loving concern for others.
In a society that profits from your self-doubt, liking yourself is a rebellious act.
I have learned the hard way never to let external factors dictate my sense of self-worth. If you needed to hear this today, you are beautiful just the way you are.
Your sheer existence is a miracle, and the sooner you accept that and start creating your life accordingly, the better.
Deciding that you are now ready to quit smoking is only half the battle. Knowing where to start on your path to becoming smoke-free can help you to take the leap. We have put together some effective ways for you to stop smoking today.
Tobacco use and exposure to second-hand smoke are responsible for more than 480,000 deaths each year in the United States, according to the American Lung Association.
Most people are aware of the numerous health risks that arise from cigarette smoking and yet, “tobacco use continues to be the leading cause of preventable death and disease” in the U.S.
Quitting smoking is not a single event that happens on one day; it is a journey. By quitting, you will improve your health and the quality and duration of your life, as well as the lives of those around you.
To quit smoking, you not only need to alter your behavior and cope with the withdrawal symptoms experienced from cutting out nicotine, but you also need to find other ways to manage your moods.
With the right game plan, you can break free from nicotine addiction and kick the habit for good. Here are five ways to tackle smoking cessation.
1. Prepare for quit day
Once you have decided to stop smoking, you are ready to set a quit date. Pick a day that is not too far in the future (so that you do not change your mind), but which gives you enough time to prepare.
There are several ways to stop smoking, but ultimately, you need to decide whether you are going to:
quit abruptly, or continue smoking right up until your quit date and then stop
quit gradually, or reduce your cigarette intake slowly until your quit date and then stop
Research that compared abrupt quitting with reducing smoking found that neither produced superior quit rates over the other, so choose the method that best suits you.
Here are some tips recommended by the American Cancer Society to help you to prepare for your quit date:
Tell friends, family, and co-workers about your quit date.
Throw away all cigarettes and ashtrays.
Decide whether you are going to go “cold turkey” or use nicotine replacement therapy (NRT) or other medicines.
If you plan to attend a stop-smoking group, sign up now.
Stock up on oral substitutes, such as hard candy, sugarless gum, carrot sticks, coffee stirrers, straws, and toothpicks.
Set up a support system, such as a family member that has successfully quit and is happy to help you.
Ask friends and family who smoke to not smoke around you.
If you have tried to quit before, think about what worked and what did not.
Daily activities – such as getting up in the morning, finishing a meal, and taking a coffee break – can often trigger your urge to smoke a cigarette. But breaking the association between the trigger and smoking is a good way to help you to fight the urge to smoke.
On your quit day:
Do not smoke at all.
Stay busy.
Begin use of your NRT if you have chosen to use one.
Attend a stop-smoking group or follow a self-help plan.
Drink more water and juice.
Drink less or no alcohol.
Avoid individuals who are smoking.
Avoid situations wherein you have a strong urge to smoke.
You will almost certainly feel the urge to smoke many times during your quit day, but it will pass. The following actions may help you to battle the urge to smoke:
Delay until the craving passes. The urge to smoke often comes and goes within 3 to 5 minutes.
Deep breathe. Breathe in slowly through your nose for a count of three and exhale through your mouth for a count of three. Visualize your lungs filling with fresh air.
Drink water sip by sip to beat the craving.
Do something else to distract yourself. Perhaps go for a walk.
Remembering the four Ds can often help you to move beyond your urge to light up.
2. Use NRTs
Going cold turkey, or quitting smoking without the help of NRT, medication, or therapy, is a popular way to give up smoking. However, only around 6 percent of these quit attempts are successful. It is easy to underestimate how powerful nicotine dependence really is.
NRT can reduce the cravings and withdrawal symptoms you experience that may hinder your attempt to give up smoking. NRTs are designed to wean your body off cigarettes and supply you with a controlled dose of nicotine while sparing you from exposure to other chemicals found in tobacco.
The U.S Food and Drug Administration (FDA) have approved five types of NRT:
skin patches
chewing gum
lozenges
nasal spray (prescription only)
inhaler (prescription only)
If you have decided to go down the NRT route, discuss your dose with a healthcare professional before you quit smoking. Remember that while you will be more likely to quit smoking using NRT, the goal is to end your addiction to nicotine altogether, and not just to quit tobacco.
Contact your healthcare professional if you experience dizziness, weakness, nausea, vomiting, fast or irregular heartbeat, mouth problems, or skin swelling while using these products.
3. Consider non-nicotine medications
The FDA have approved two non-nicotine-containing drugs to help smokers quit. These are bupropion (Zyban) and varenicline (Chantix).
cravings and withdrawal symptoms.
Talk to your healthcare provider if you feel that you would like to try one of these to help you to stop smoking, as you will need a prescription.
Bupropion acts on chemicals in the brain that play a role in nicotine craving and reduces cravings and symptoms of nicotine withdrawal. Bupropion is taken in tablet form for 12 weeks, but if you have successfully quit smoking in that time, you can use it for a further 3 to 6 months to reduce the risk of smoking relapse.
Varenicline interferes with the nicotine receptors in the brain, which results in reducing the pleasure that you get from tobacco use, and decreases nicotine withdrawal symptoms. Varenicline is used for 12 weeks, but again, if you have successfully kicked the habit, then you can use the drug for another 12 weeks to reduce smoking relapse risk.
Risks involved with using these drugs include behavioral changes, depressed mood, aggression, hostility, and suicidal thoughts or actions.
4. Seek behavioral support
The emotional and physical dependence you have on smoking makes it challenging to stay away from nicotine after your quit day. To quit, you need to tackle this dependence. Trying counseling services, self-help materials, and support services can help you to get through this time. As your physical symptoms get better over time, so will your emotional ones.
Combining medication – such as NRT, bupropion, and varenicline – with behavioral support has been demonstrated to increase the chances of long-term smoking cessation by up to 25 percent.
Behavioral support can range from written information and advice to group therapy or individual counseling in person, by phone, or online. Self-help materials likely increase quit rates compared with no support at all, but overall, individual counseling is the most effective behavioral support method.
The National Cancer Institute (NCI) provide help to anyone who wants to stop smoking through their support services:
smoking helpline: 1-877-44U-QUIT (1-877-448-7848)
local and state quitlines: 1- 800-QUIT-NOW (1-800-784-8669)
LiveHelp online chat
Smokefree website
SmokefreeTXT text messaging service
Twitter
Facebook
Instagram
Support groups, such as Nicotine Anonymous (NicA), can prove useful too. NicA applies the 12-step process of Alcoholics Anonymous to tobacco addiction. You can find your nearest NicA group using their website or by calling 1-877-TRY-NICA (1-877-879-6422).
5. Try alternative therapies
Some people find alternative therapies useful to help them to quit smoking, but there is currently no strong evidence that any of these will improve your chances of becoming smoke-free, and, in some cases, these methods may actually cause the person to smoke more.
Some alternative methods to help you to stop smoking might include:
cessation.
filters
smoking deterrents
electronic cigarettes (e-cigarettes)
tobacco strips and sticks
nicotine drinks, lollipops, straws, and lip balms
hypnosis
acupuncture
magnet therapy
cold laser therapy
herbs and supplements
yoga, mindfulness, and meditation
E-cigarettes
E-cigarettes are not supposed to be sold as a quit smoking aid, but many people who smoke view them as a method to give up the habit.
E-cigarettes are a hot research topic at the moment. Studies have found that e-cigarettes are less addictive than cigarettes, that the rise in e-cigarette use has been linked with a significant increase in smoking cessation, and that established smokers who use e-cigarettes daily are more likely to quit smoking than people who have not tried e-cigarettes.
The gains from using e-cigarettes may not be risk-free. Studies have suggested that e-cigarettes are potentially as harmful as tobacco cigarettes in causing DNA damage and are linked to an increase in arterial stiffness, blood pressure, and heart rate.
Quitting smoking requires planning and commitment – not luck. Decide on a personal plan to stop tobacco use and make a commitment to stick to it.
Weigh up all your options and decide whether you are going to join a quit-smoking class, call a quitline, go to a support meeting, seek online support or self-help guidance, or use NRTs or medications. A combination of two or more of these methods will improve your chances of becoming smoke-free.
In addition to trying out these steps, you could check out our selection of the best apps for quitting smoking.
https://moreliaclinic.com/wp-content/uploads/2015/08/FINAL-MORELIA-LOGO1.png00adminhttps://moreliaclinic.com/wp-content/uploads/2015/08/FINAL-MORELIA-LOGO1.pngadmin2020-01-13 21:49:002020-01-13 21:49:03Five ways to quit smoking
In this special feature, we collate some of the most intriguing hypertension studies from 2019. We particularly focus on nutrition, risk factors, and hypertension’s relationship with dementia.
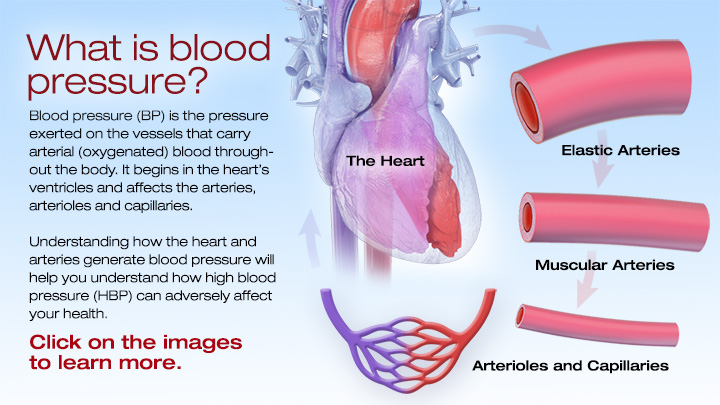
Today, in the United States, around 1 in 3 adults has high blood pressure, which doctors also call hypertension.
Hypertension increases the risk of cardiovascular events, such as stroke and coronary disease, and, if doctors don’t treat it, it can reduce lifespan.
Because it is worryingly prevalent, and because the physical ramifications can be significant, scientists are plowing a great deal of effort into understanding hypertension.
Although people first identified hypertension as a medical condition thousands of years ago, scientists are still picking away at the details.
Research that scientists completed in 2019 has thrown out some exciting and, in some cases, unexpected findings. For instance, a paper appearing in February concluded that, for women over 80 years of age, having “normal” blood pressure had an increased risk of mortality when compared with individuals with high blood pressure.
Elsewhere, Greek scientists concluded that napping might help reduce blood pressure. “Midday sleep appears to lower blood pressure levels at the same magnitude as other lifestyle changes,” explains one of the researchers, Dr. Manolis Kallistratos.
Another surprising study, which scientists presented at the 83rd Annual Scientific Meeting of the Japanese Circulation Society, concluded that needing to urinate multiple times at night might be a sign of hypertension.
The role of nutrition
The food that we eat has a huge impact on our overall health; that goes without saying. The America Heart Association, for instance, suggest that eating a diet rich in fruits and vegetables and avoiding products with high levels of salt and fat can help keep blood pressure in check.
Over the past few years, interest in nutrition, in general, has skyrocketed. More and more, scientists are focusing on individual foods or food compounds that can directly benefit health. So, although poor diet is a well-known risk factor for hypertension, researchers in 2019 drilled down deeper.
Specific foods and supplements
One study appearing in 2019 investigated the impact of consuming walnuts on blood pressure. It concluded that the individuals who ate an experimental walnut-heavy diet experienced a significant reduction in blood pressure.
In these types of studies, it is worth digging a little deeper; often, industry or organizations who might stand to benefit from positive results are funding them. The walnut study above, for instance, was partly funded by the California Walnut Commission.
This observation does not mean that we should dismiss the results out of hand, but it provides pause for thought.
Another recent study concentrated on spirulina, which is the dried biomass of a bacterium called Spirulina platensis. Manufacturers can add it to foods, and some people take it as a supplement.
Earlier experiments hinted at spirulina’s potential to reduce hypertension, and in the most recent study, they attempted to find out why this might be.
The scientists concluded that a protein that the digestion of spirulina produces causes blood vessels to relax. The authors hope that this protein, known as SP6, might one day be useful in the treatment of hypertension.
Preservatives, additives, and water
Rather than focus on specific foods, a further study looked at the impact of buying food from local retailers rather than supermarkets.
The authors theorized that by eating local produce, individuals would avoid consuming the various preservatives and additives that keep food “fresh” over long distances.
Although the study was relatively small, the authors found that after 6 months, those who consumed local produce had lower levels of visceral fat, improved depression scores, and reduced systolic blood pressure.
Approaching from a different angle, a team of scientists recently asked whether drinking water that is high in minerals might reduce blood pressure.
To investigate, they focused on people living in a coastal region of Bangladesh. Drinking water there varies in salinity. In areas of high salinity, the water contains greater quantities of sodium, which we know increases blood pressure. However, the same water also includes more magnesium and calcium, both of which reduce blood pressure.
The authors concluded that higher salinity levels decreased blood pressure overall; they write that “the [blood pressure]-lowering effects of [calcium] and [magnesium] counteracted the harmful effects of [sodium].
Causes and risk factors
Some risk factors for hypertension are fairly well established; they include drinking excessive amounts of alcohol, smoking tobacco, stress, and obesity. However, because high blood pressure is so common, there are likely to be many more factors at play.
Similarly, although scientists know which lifestyle and dietary factors influence blood pressure, they are not entirely sure how they cause the changes.
Understanding why and how blood pressure arises in some people and not others is essential and could, potentially, lead to innovative ways of treating or preventing hypertension.
Some scientists are exploring possible risk factors which, at face value, seem unlikely. For instance, one paper, appearing in the Journal of Public Health in June, examined the role of where people live.
Earlier studies found an association between exposure to air pollution and hypertension risk, and this latest work confirms those earlier suspicions and takes it a step further.
As expected, the researchers found a relationship between air pollution and hypertension; however, the increase in risk was only significant for those who were living in multi-family homes, such as blocks of flats.
The authors believe that this might be due to several factors, for instance, living in close quarters with other people may be more stressful or more noisy. This study provides a glimpse of the complex realm of potential elements that might influence blood pressure.
Oral hygiene
Bizarrely, one group of scientists recently investigated how mouthwash might influence hypertension risk.
Publishing their findings in the journal Frontiers in Cellular and Infection Microbiology, the authors conclude that mouthwash kills “good bacteria” in the mouth. These good bacteria produce nitric oxide (NO), which is important for blood vessel health.
NO acts as a vasodilator, which means it causes the muscles that line blood vessels to relax, thereby widening the vessels and reducing blood pressure.
In particular, the scientists concentrated on the chemical chlorhexidine, which they found in some mouthwashes.
According to the authors, they demonstrated that “twice-daily chlorhexidine usage was associated with a significant increase in systolic blood pressure after 1 week of use, and recovery from use resulted in an enrichment in nitrate-reducing bacteria on the tongue.”
Still focusing on the oral region, a 2019 review looked for links between gum disease and hypertension. They showed that individuals with severe periodontitis — a form of gum disease — had a 49% increased risk of hypertension.
Senior author Prof. Francesco D’Aiuto explains their results in a nutshell: “We observed a linear association — the more severe periodontitis is, the higher the probability of hypertension.”
The role of zinc
Another project investigated the role of zinc in maintaining blood pressure at healthy levels. Over the years, researchers have noted links between low zinc levels and an increased risk of high blood pressure, but the precise mechanism has been tough to pin down.
The latest research identified the key player in this interaction between zinc and blood pressure; according to the authors, the sodium chloride cotransporter (NCC) in the kidney is the lynchpin. The NCC is responsible for pumping sodium back into the body, thereby preventing it from being excreted in the urine.
Zinc interacts with the NCC: when zinc is present, the NCC is less active, meaning that the body retains less sodium. This is important because high sodium levels — from consuming too much salt, for instance — are factors in increasing the risk of hypertension.
The authors hope that this new knowledge will help improve treatment and write:
“Understanding the specific mechanisms by which [zinc deficiency] contributes to [blood pressure] dysregulation may have an important effect on the treatment of hypertension in chronic disease settings.”
Hypertension and dementia
Scientists have identified a relationship between hypertension and vascular dementia. The association makes sense because vascular dementia can occur following stroke, and hypertension is a risk factor for stroke.
However, it also appears that hypertension might increase the risk of other types of dementia, including Alzheimer’s disease.
A study appearing in June this year found that a common blood pressure drug — nilvadipine — slowed the progress of Alzheimer’s disease by improving blood flow in the brain.
Specifically, the research team showed that people who took the medication had a 20% increase in blood flow in the hippocampus, a brain region vital for memory and learning, in comparison to those who did not take nilvadipine.
Patterns throughout life
Other scientists have looked at fluctuations in blood pressure and their possible role in dementia. For instance, one investigation that recruited participants who were living with Alzheimer’s disease found that the condition progressed quicker in those whose blood pressure fluctuated most.
“More fluctuations [in blood pressure] might affect whether cognitive function declines more slowly or rapidly.”
Senior author Dr. Jurgen Claassen
With a similar theme, another group of scientists observed the pattern of blood pressure across decades. The authors summarize their findings:
“[A] pattern of sustained hypertension from middle to late life and a pattern of midlife hypertension followed by late-life hypotension were associated with an increased risk for subsequent dementia, compared with participants who maintained normal blood pressure.”
Another project that charted hypertension over a lifespan found that individuals with high or rising blood pressure between 36 and 53 years of age were more likely to have white matter lesions and a smaller brain volume in later life.
The authors hope that these findings will inspire both doctors and the public to check and take charge of their blood pressure sooner rather than later.
As 2020 rolls into view, hypertension is sure to stay high on the medical research agenda. As science gradually untangles hypertension’s causes and mechanisms, managing and minimizing this highly prevalent condition must draw ever closer.
https://moreliaclinic.com/wp-content/uploads/2015/08/FINAL-MORELIA-LOGO1.png00adminhttps://moreliaclinic.com/wp-content/uploads/2015/08/FINAL-MORELIA-LOGO1.pngadmin2020-01-06 21:16:162020-01-06 21:16:18High blood pressure research
Do we make New Year’s resolutions just to ignore them? Are they merely promises doomed to fail? In this feature, we ask whether, statistically speaking, these resolutions work, and what increases the chances of success.
New Year’s resolutions are an ancient tradition that continues to this day.
The Babylonians started each year with pledges to pay debts and return borrowed items.
The Romans began their year by promising the two faced god, Janus, that they would behave better.
In modern societies, many people still promise to make changes as the new year dawns; this desire, in many cases, is fueled by the excesses of the holiday period.
Most commonly, it would seem, New Year’s resolutions revolve around weight loss, quitting smoking, reducing drinking, and exercising more.
How effective are annual resolutions?
A study from 1989 tracked 200 people living in Pennsylvania as they attempted to make changes based on New Year’s resolutions.
On average, the participants made 1.8 resolutions, most commonly, to stop smoking or lose weight. Less frequently, people pledged to improve relationships, and a surprisingly low 2.5% were hoping to control their drinking habits.
An impressive 77% managed to hold to their pledges for 1 week, but the success rate dropped to 19% over 2 years. Although that is a substantial drop out rate, it means that 1 in 5 of those participants achieved their goal.
Of the 77% successful resolvers, more than half slipped at least once, and, on average, people slipped 14 times across the 2 years.
A study in the Journal of Consulting and Clinical Psychology in 1988 followed the efforts of 153 New Year’s resolvers who were determined to quit smoking.
At 1 month, 77% of participants had managed at least one 24-hour period of abstinence. Overall, though, the results seemed a little disappointing with the authors writing:
“Only 13% of the sample was abstinent at 1 year, and 19% reported abstinence at the 2-year follow-up.”
Another study, appearing in PLOS ONE, took a more general look at behavior. The research team tracked the food shopping habits of 207 households from July 2010 to March 2011.
Unsurprisingly, the researchers found that, during the holiday period, expenditure increased by 15%. Three-quarters of this increase went on less healthful items.
Also, as expected, when January rolled around, the sale of healthful items shot up by 29.4%.
However, the sale of less healthful items did not drop in tandem with this health drive — people were buying more nutritious items, but still purchasing the same amount of unhealthful food.
Overall, the number of calories they purchased in the New Year was higher than during the holiday period. The authors conclude:
“Despite resolutions to eat more healthfully after New Year’s, consumers may adjust to a new ‘status quo’ of increased less-health[ful] food purchasing during the holidays, and dubiously fulfill their New Year’s resolutions by spending more on health[ful] foods.”
The authors believe that the key to successful resolutions is to focus on replacing unhealthful items with healthful ones, rather than buying both.
That is sound advice, but not necessarily easy to implement.
Successes and failures of weight loss goals
In 2009, GlaxoSmithKline released Orlistat, which they hailed as “the first clinically proven over-the-counter weight loss aid” in Europe.
As part of their marketing push, the company also conducted an internet survey about weight loss that included questions about New Year’s resolutions.
Although the survey was not meant to be a scientific study, it generated a substantial pool of data with 12,410 females from six European countries responding.
A group of researchers took advantage of this dataset and published an analysis in the journal Obesity Facts.
They found that around half of the women had made a weight loss New Year’s resolution in the past 2 years.
As for success rates, they observed that women with a body mass index (BMI) of under 25, which health experts define as “normal,” were successful 20% of the time.
However, of thos with a BMI of 30 or above — which doctors class as overweight or obese — only 9% reported some success.
In the overweight group, three-quarters of the female respondents said that their primary reason for failing to lose weight was that it took too long to see results. Around one-third of those who were obese or overweight stated that they were not successful due to a lack of confidence.
What increases the chances of succeeding?
In the Pennsylvania study we mention above, the scientists found no link between success rate and participants’ sex or age; similarly, the type of resolution did not influence how likely they were to succeed.
The researchers contacted participants by telephone after 1 week, 1 month, 3 months, 6 months, and 2 years.
During these interviews, the researchers also asked participants what techniques they used to help them keep their resolutions, and how often they implemented each one.
They found that the most successful resolvers were applying stimulus control at all five checkpoints.
Stimulus control is the act of keeping things around you that remind you why you chose the resolution.
For instance, someone who is quitting smoking might keep a picture of their young child nearby to remind them why they decided to stop.
At the 6-month and 2-year mark, successful resolvers were using self-liberation (or willpower), and reinforcement management — rewarding themselves for being successful.
Conversely, individuals who did not keep their resolutions most commonly employed self-blame and wishful thinking.
The study we highlighted above that followed the fates of 153 smokers also looked at factors that made quitting more likely. The authors explain:
“The use of multiple strategies for cessation was associated with abstinence at the 2-year follow-up. A strong motivation to quit was found to be important for both initial success and long-term maintenance.”
Other studies that have investigated smoking cessation more generally have identified factors that increase the chance of quitting. These factors include staying away from smokey environments, abstaining from alcohol, stress management techniques, and will power.
Another paper took a different approach. Publishing their work in the Journal of Clinical Psychology, the authors set out to understand why some people succeeded where others failed.
To do this, they recruited two sets of participants: 159 New Year’s resolvers and 123 people who were interested in solving a problem at a later date. The researchers followed the participants for 6 months and charted their successes and failures.
In agreement with other studies, the most common reasons for New Year’s resolutions were losing weight, increasing exercise, and quitting smoking.
The authors found that the most successful resolvers used more willpower, stimulus control, reinforcement management, positive thinking, and avoidance strategies.
Conversely, those who were less successful tended to use more wishful thinking, blame and criticize themselves, and make light of the problem.
Ending on a high
Some of the results above might cast a shadow across ambitions to make a change in 2020, but they shouldn’t.
The authors of the study above made some overarching conclusions that should boost the confidence of any New Year’s resolver:
“Resolvers reported higher rates of success than nonresolvers; at 6 months, 46% of the resolvers were continuously successful compared to 4% of the nonresolvers.”
So, although the cards might be stacked against anyone who plans to make a New Year’s resolution, simply by making that resolution, you have boosted your odds of success.
According to this data, forming a New Year’s resolution increases your chances of generating change more than 10-fold.
The authors write that, “Contrary to widespread public opinion, a considerable proportion of New Year resolvers do, in fact, succeed, at least in the short run.”
In conclusion, New Year’s resolutions do not work for everyone. But, as the saying goes, “you’ve got to be in it to win it.”
If you are considering making a resolution for 2020, according to the findings of these studies, the best approach is to keep things around you to remind you why you want to make those changes.
Also, reward yourself for successes, and stay motivated. Throw a healthful dose of willpower into the seasonal mix, and you are likely to succeed. Good luck!
https://moreliaclinic.com/wp-content/uploads/2015/08/FINAL-MORELIA-LOGO1.png00adminhttps://moreliaclinic.com/wp-content/uploads/2015/08/FINAL-MORELIA-LOGO1.pngadmin2020-01-02 20:46:452020-01-02 20:46:47New Year’s resolutions: How to boost success rates
A recent study concludes that people who smoke electronic cigarettes are twice as likely to report clinical depression as those who have never vaped. The correlation was particularly strong among younger people.
Known as vaping, battery-powered e-cigarettes use heat to deliver an aerosol cocktail of nicotine and flavors to the user. An e-cigarette produces a small cloud of vapor, whereas a cigarette releases smoke.
Many people believe that the vapor contains water. In fact, it contains varying amounts of toxic chemicals that have links to heart and respiratory diseases, as well as cancer.
The use of e-cigarettes in the United States has snowballed since their introduction a decade ago.
According to the Annals of Internal Medicine
in 2016, an estimated 10.8 million people in the U.S. used e-cigarettes. Of this number, 2.8 million (9.2%) were 18–24 years old.
Today, some experts consider vaping to be an epidemic among teenagers — the number of high school students who turned to vaping doubled in 2018.
Although links between traditional cigarettes and depression primarily prompted the study, the results of an earlier study that indicated that 9.1% of those with depression were e-cigarette users, compared with 4.5% among the general population was also a factor.
First author of the study, Dr. Olufunmilayo Obisesan of John Hopkins University in Baltimore, MD, told Medical News Today that “Combustible cigarette smoking has been linked with an increased risk of developing major depressive disorder and has also been shown to be highly predictive of future suicidal behavior among individuals with a history of depression.”
“In light of the similarities in some of the constituents of cigarettes and e-cigarettes, we decided to explore the existence of a similar association between e-cigarettes and depression.”
Concerns for youngsters who vape
The study looked at the responses of nearly 900,000 randomly sampled adults aged 18 and older in a cross-sectional study of 2016–2017 data gathered by the Behavioral Risk Factor Surveillance System (BRFSS)
The BRFSS is the largest national telephone survey carried out in the U.S.
“The researchers found that 34% of current e-cigarette users reported having experienced clinical depression, compared with 15% of those who had never vaped. Also, 27% of former users were more likely to report clinical depression, compared with 15% in those who had never used e-cigarettes.
College students aged 18–25 showed the most significant link between e-cigarette use and depression.
The scientists focused on this group in particular because, typically, young people are more likely to experiment with new products, such as e-cigarettes. Tobacco companies often target this demographic in marketing campaigns.
“This highlights the potential susceptibility of e-cigarette users in this group to depression at a particularly vulnerable time in their lives, but also warrants pause in what this kind of nicotine addiction may be doing to our children, high schoolers, and younger, who we know are using e-cigarettes in epidemic proportions,” says Dr. Mariell Jessup of the American Heart Association’s (AHA) Tobacco Center of Regulatory Science.
The AHA has launched a major initiative to tackle youth e-cigarette use and nicotine addiction.
“The main implication of our findings for the youth is that they need to know that there are potential mental health effects associated with the use of e-cigarettes.”
Dr. Olufunmilayo Obisesan
Depression risk rises with increased use
The study also found that the link between e-cigarette use and depression was stronger in people who vaped the most often.
“Clinically, our study provides information that physicians could consider when counseling patients seeking information about e-cigarettes, especially those with depression,” Dr. Obisesan told MNT.
He added that the study emphasized the need for doctors and health professionals to routinely collect information on e-cigarette from individuals during clinic visits, especially among those with mental health conditions. In conclusion, Dr. Obisesan told MNT:
“We hope that our study will provide a baseline for future longitudinal studies that can confirm our findings and establish the direction of association between e-cigarette use and depression, which we currently believe to be bi-directional.”
https://moreliaclinic.com/wp-content/uploads/2015/08/FINAL-MORELIA-LOGO1.png00adminhttps://moreliaclinic.com/wp-content/uploads/2015/08/FINAL-MORELIA-LOGO1.pngadmin2019-12-16 21:26:132019-12-16 21:26:16A new study identifies a link between vaping and depression.
Researchers using a new method of assessing risk factors for prostate cancer have found an intriguing link between a lack of physical activity and an increased risk of this condition.
According to data from the National Cancer Institute (NCI), by the end of 2019, there will have been an estimated 174,650 new cases of prostate cancer in the U.S. alone.
Despite the number of people that this cancer affects every year, specialists still have insufficient knowledge about the risk factors that may play a role in its development.
The NCI cite a mix of modifiable and nonmodifiable factors, including age, a family history of prostate cancer, and the levels of vitamin E, folic acid, and calcium in the body.
Yet there may be other lifestyle-related factors at play, and investigators are hard at work to uncover them.
Recently, a team of researchers from the University of Bristol and Imperial College London in the United Kingdom — alongside colleagues from other academic institutions across the globe — have used a different approach to try to find out more about prostate cancer risk factors.
In their new study, the findings of which now appear in the International Journal of Epidemiology, the investigators used a method called “Mendelian randomization.”
Mendelian randomization
allows researchers to look at genetic variations to assess causal relationships between various potential risk factors and the development of certain outcomes — in this case, prostate cancer.
Physical activity may more than halve risk
In their study, the researchers identified potential risk factors for prostate cancer through the World Cancer Research Fund’s (WCRF) 2018 systematic review of the evidence.
They also had access to the medical information of 79,148 participants with prostate cancer, as well as 61,106 participants without cancer who acted as the controls.
The analysis revealed that individuals with a genetic variation that increased their likelihood of being physically active had a 51% lower risk of prostate cancer than people who did not have this genetic variation.
Moreover, the researchers explain that “physical activity,” in this case, refers to all forms of activity, not just exercise.
Following on from this, the study authors conclude that interventions encouraging males to ramp up their levels of physical activity may have a protective effect against this widespread form of cancer.
“This study is the largest-ever of its kind, which uses a relatively new method that complements current observational research to discover what causes prostate cancer,” notes study co-author Sarah Lewis, Ph.D.
“It suggests that there could be a larger effect of physical activity on prostate cancer than previously thought, so will hopefully encourage men to be more active.”
Sarah Lewis, Ph.D.
Anna Diaz Font, who is head of research funding at WCRF — which, alongside Cancer Research U.K., funded this study — emphasizes the importance of the current findings.
“Up till now, there has only been limited evidence of an effect of physical activity on prostate cancer. This new study looked at the effect of 22 risk factors on prostate cancer, but the results for physical activity were the most striking,” she says.
The study’s findings, Diaz Font believes, “will pave the way for even more research, where similar methods could be applied to other lifestyle factors, to help identify ways men can reduce their risk of prostate cancer.”
https://moreliaclinic.com/wp-content/uploads/2015/08/FINAL-MORELIA-LOGO1.png00adminhttps://moreliaclinic.com/wp-content/uploads/2015/08/FINAL-MORELIA-LOGO1.pngadmin2019-12-09 20:44:262019-12-09 20:44:28New evidence suggests that being physically active could help slash prostate cancer risk.
Both flu (influenza) and cold are caused by viruses, and they can have similar symptoms. So how do we know if a person has the flu or a bad cold? In this article, we explain the differences.
Cold and influenza are the most common illnesses in humans.
. Every year, 5-20 percent of the population of America develop flu symptoms.
The main difference between cold and flu is that, generally, symptoms of the flu are usually a lot more severe.
Each year, more than 200,000 people are hospitalized because of flu complications; flu is responsible for around 23,600 deaths every year.
Fast facts on colds vs. flu:
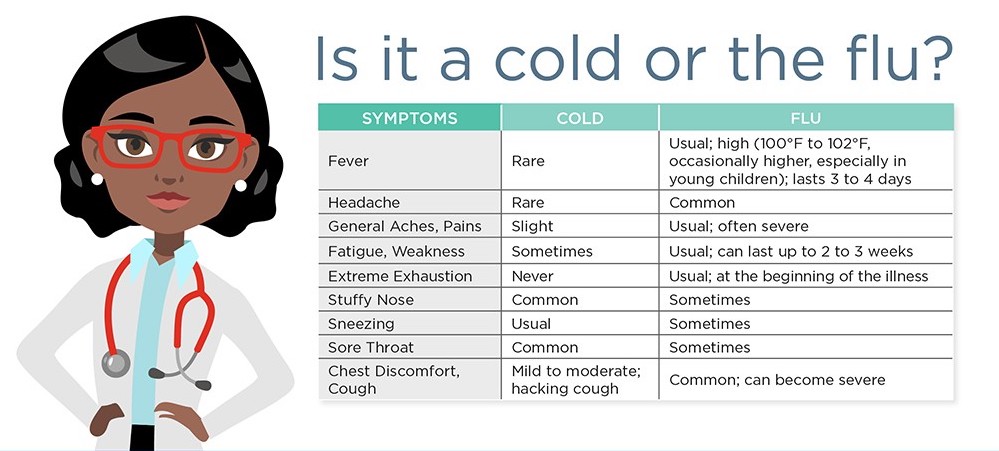
Colds and flu share many of the same symptoms; the major difference being flu is often worse, and accompanied by a high fever.
According to the Centers for Disease Control and Prevention (CDC), the average adult will have 2-3 colds every year.
The rhinovirus is the most common cause of cold.
The difference between cold and flu
Cold and flu are caused by different viruses, and, in general, the symptoms of flu are worse. Also, there are less likely to be serious complications from cold, such as pneumonia and bacterial infections.
The main difference between cold and flu symptoms is that flu more commonly includes fever; the fever can be 100 degrees Fahrenheit or higher and last for 3-5 days.
The extreme fatigue associated with flu can persist for weeks. Cold symptoms are generally milder and last about 1 week.
Also, runny nose or nasal congestion is more common with cold than flu.
Vomiting is another key difference; vomiting is not normally associated with the common cold but can be present in flu.
Although the differences above are generally true, without conducting special tests, it is impossible to know for sure whether it is flu or cold. For instance, it is possible to have flu without fever.
What is a cold?
Almost everybody is familiar with the sensation of having a cold. Colds affect both warm and cool climates equally, and the average person will have had many colds from infancy all the way until later life.
Symptoms include a runny nose, sore throat, coughing and sneezing, watery eyes, a headache, and body aches. There is no cure, except for resting and drinking plenty of fluids, but the cold should pass within 7-10 days.
There is normally no need to visit a doctor, but a person with a weakened immune system is more prone to developing pneumonia as a complication
To avoid catching or spreading a cold, people should wash their hands regularly and make sure they sneeze into a tissue or handkerchief, or into their elbow. This is the most hygienic as it stops the spread of germs, which cannot live on clothing or surfaces like they can on skin.
What is flu?
There are three types of flu virus, influenza A, influenza B, and influenza C. Types A and B are the ones that cause seasonal epidemics. One of the key symptoms of flu is feeling feverish or having a temperature of 100 degrees Fahrenheit or above. However, not everyone with the flu will have a fever.
Other symptoms include:
headaches or body aches
vomiting, nausea, and possibly diarrhea, especially in children
a sore throat and a cough
fatigue
chills and shivering
a congested or runny nose
A common cold is less likely to cause a high fever. With a cold, symptoms such as a runny nose or throat irritation will normally improve within a few days.
How to treat flu
The CDC note that the majority of people who have the flu do not need medical attention. Most can remain at home and avoid contact with other people to prevent the disease from spreading. However, the following treatments are available:
Over-the-counter medications – these can reduce fever. Tylenol can help people with flu feel more comfortable while they recover. Tylenol is also available to purchase online.
Prescription antiviral flu drugs – these are also available from a physician. They are for people who are at high risk of serious complications and are not normally necessary for effective treatment. They can only be given within a certain amount of time from symptom onset.
Home remedies – to alleviate symptoms, home remedies such as steam inhalation, nourishing foods like chicken soup, keeping warm, and other comfort measures can be used.
A physician will be able to decide if antivirals are needed. People who tend to be at greater risk include infants under the age of 2, people aged 65 years and older, and pregnant women.
Emergency warning signs for flu
Patients should seek medical help if they notice any of the emergency warning signs.
Warning signs in infants include difficulty breathing, having no appetite, and not producing tears when they cry, or having fewer wet diapers than usual.
Severe symptoms in older children include:
breathing problems
bluish skin color
not drinking enough fluids
not waking up or interacting
being so irritable that they do not want to be held
fever with a rash
If flu-like symptoms improve but then return with fever and a worse cough, the parent should consult a physician.
Anti-flu vaccines and other types of protection
The best way to protect against the flu is by having an annual vaccination, as this helps the body to build up the immune system so that it can fight off the virus more quickly.
The flu vaccine is recommended during pregnancy as it has been proven safe. If flu occurs during pregnancy, it can have serious complications for the unborn child and the mother.
https://moreliaclinic.com/wp-content/uploads/2015/08/FINAL-MORELIA-LOGO1.png00adminhttps://moreliaclinic.com/wp-content/uploads/2015/08/FINAL-MORELIA-LOGO1.pngadmin2019-12-02 19:51:462019-12-02 19:51:48What is the difference between cold and flu?
Vulvodynia and vestibulodynia refer to a chronic discomfort of the vulva, the part of a woman’s body that protects the genitals.
It includes the external female genitalia, including the mons pubis, the labia majora and minora, the clitoris, and the perineum.
Vulval pain can happen for a number of reasons, but vulvodynia and vestibulodynia are specifically linked to a hypersensitivity of the nerve endings in the skin.
Around 16 percent of women are estimated to have experienced pain or stinging in the vulval area at some time in their life.
Treatment
Treatment aims to alleviate symptoms. As the cause is unknown, finding a solution that works may take some trial and error.
Medications to block pain may include antidepressants, anticonvulsants, or serotonin-norepinephrine reuptake inhibitors (SNRIs).
Other solutions include creams, lotions, and anesthetic gel for applying to the vulval area.
Examples include topical hormone creams containing estrogen and testosterone, topical anesthetics, such as lidocaine, and products that contain an antidepressant or anticonvulsant ingredient. These can be applied 15 to 20 minutes before sexual activity, or when needed. Some of these products are available for purchase online, including lidocaine.
A nerve block is an anesthetic drug that is injected into the nerves that transmit pain signals, in this case, from the vulva to the spine. Interrupting the pain signals in this way can provide short-term relief.
If no other method is effective, surgery to remove the painful tissue may be appropriate.
Two techniques that are currently being investigated are neurostimulation and the spinal infusion pump.
Neurostimulation involves delivering low-voltage electrical stimulation to a specific nerve. This can replace pain with a tingling sensation.
A spinal infusion pump is an implanted device that can deliver low-dose medication to the spinal cord and nerve roots. This can dull pain.
However, there is limited evidence regarding the use of these measures for vulvodynia.
Some researchers have found that physical and psychosexual therapy can help improve sexual functioning, for example, by helping to reverse a fear of touch.
Symptoms
Vulvodynia features a burning, stinging, itching, irritating, or a raw feeling in the vulvar tissue, which may or may not appear inflamed. Patients may describe a feeling of throbbing, itching, aching, soreness, and swelling.
The pain can affect a particular spot, or it may be felt in a wider area, including the clitoris, the perineum, the mons pubis, and the inner thighs. It can also affect the area around the urethra and the top of the legs and inner thighs.
The pain involved in vulvodynia is neuropathic, which means it stems from abnormal signals from the nerve fibers in the vulval area. The nerve endings are hypersensitive.
It may be constant or intermittent. A constant pain that happens when there is no touch or pressure is known as unprovoked vulvodynia.
Vestibulodynia, previously known as vestibulitis, involves a pain that is triggered by light touch, or provoked pain.
Symptoms may be worse during or after sexual intercourse, walking, sitting, or exercising. It can happen when inserting a tampon, or when prolonged pressure is applied, for example, during horseback riding.
Vulvodynia is usually defined as lasting for at least 3 months. It often starts suddenly, and it may last for months or years. It is not life-threatening, but the pain can prevent the individual from carrying out some normal activities. This can also lead to upset or depression.
Complications
Relationship problems can result, because sexual intercourse is painful. One study suggests that 60 percent of women with vulvodynia are unable to engage in sex.
Studies suggest
that women who have vulvodynia can have a normal pregnancy, and that in some cases, pain levels fall during pregnancy. However, women with the condition are more likely to have a cesarean delivery.
Home remedies
Some measures can be taken that do not involve medications.
If vulvodynia occurs, the first step is to stop using any irritants, such as perfumed soaps. A change in menstrual products might help, for example, switching from synthetic to cotton-based items.
Cool gel packs may offer immediate, short-term pain relief. A range of cool gel packs is available for purchase online.
Pelvic floor muscle exercises may help by relaxing tissues in the pelvic floor and releasing tension in muscles and joints.
Biofeedback uses technology to increase an individual’s awareness of how they might be stressing their body. This information can help people change habits that lead to harm or discomfort. For women with vulvodynia, it can help strengthen the pelvic floor muscles, and this may reduce pain.
A trigger point is a specific area of discomfort. Trigger-point therapy involves massaging a small area of tightly contracted muscle to release tension and relieve pain. An anesthetic medication applied directly, for example, as a cream, can also be used to relieve pain in a trigger point.
Since stress can play a role in vulvodynia, either as a trigger or a consequence, stress management may help ease symptoms.
Acupuncture and cognitive behavior therapy are options currently being explored.
Diet
A change in diet may help. Cutting out one food at a time may help to pinpoint a trigger.
Items that commonly trigger a reaction include:
caffeine
high-sugar foods
acidic foods
processed foods
Causes
Vulvar pain can be caused by infections, neurological problems, inflammatory conditions, and neoplasms, such as squamous cell carcinoma.
Vulvodynia is not related to an underlying condition. The exact cause is unknown. It is not caused by a sexually transmitted or other infection, skin disease, or cancer, although these can also cause pain.
Factors that may raise the risk of vulvodynia include:
Damage to or irritation of the nerves around the vulva
A high density of pain-sensing nerve fibers in the vulval area
High levels of inflammatory substances in the vulval area, for example, because of inflammation
genetic susceptibility
pelvic floor muscles are weak or unstable
unusual or long-term reaction to infection, trauma, or another environmental factor
changes triggered by hormones
Other factors that increase susceptibility include:
frequent yeast infections
sexually transmitted infections (STIs)
chemical irritation of the external genitals, caused by soaps, feminine hygiene products or detergents in clothing
rashes on the genital area
previous laser treatments or surgery on the external genitals
nerve irritation, injury or muscle spasms in the pelvic area
diabetes
precancerous or cancerous conditions on the cervix
Provoked vestibulodynia could result from:
sexual intercourse
tampon insertion
a gynecologic examination
prolonged sitting
wearing tight underclothes or pants
activities such as cycling or horseback riding
Clitorodynia refers to pain in the clitoris.
Vulvodynia can be confused with other vulvovaginal problems, such as chronic tension or spasm of the muscles of the vulvar area called vaginismus.
Prevention
Measures that can reduce the risk of triggering pain include:
wearing cotton underwear and loose-fitting clothes around the genital area
avoiding scented toilet paper and perfumed creams and soaps
avoiding friction or sitting for prolonged periods
refraining from excessive genital washing
not douching or using vaginal wipes
using water-soluble lubricants during sexual intercourse
patting the area dry after rinsing or urinating
If a vaginal infection is suspected, it is important to have it diagnosed and treated promptly and to discuss with a physician if any treatments appear to make the condition worse.
Diagnosis
Diagnosis may involve a pelvic exam, to look for skin changes and assess the pain.
A cotton swab test is used to delineate the areas of pain and categorize their severity. The physician may press with swab on different areas while asking the patient to rate the level of pain.
The patient should be ready to describe the pain, including the type of pain and its severity, say when it started, and whether it began gradually or suddenly, where it hurts, and how often.
The doctor may use a special magnifying glass, to carry out a colposcopy.
Tests may be carried out to try to find the source of the pain and to eliminate other causes.
These include:
taking a culture for bacteria and yeast
blood tests to assess levels of estrogen, progesterone, and testosterone
a biopsy
In a biopsy, the doctor first numbs the genital area with a painkiller, and then a small piece of tissue is taken for examination under a microscope.
https://moreliaclinic.com/wp-content/uploads/2015/08/FINAL-MORELIA-LOGO1.png00adminhttps://moreliaclinic.com/wp-content/uploads/2015/08/FINAL-MORELIA-LOGO1.pngadmin2019-11-25 19:45:132019-11-25 19:45:16Vulvodynia: What you need to know