Researchers using a new method of assessing risk factors for prostate cancer have found an intriguing link between a lack of physical activity and an increased risk of this condition.
According to data from the National Cancer Institute (NCI), by the end of 2019, there will have been an estimated 174,650 new cases of prostate cancer in the U.S. alone.
Despite the number of people that this cancer affects every year, specialists still have insufficient knowledge about the risk factors that may play a role in its development.
The NCI cite a mix of modifiable and nonmodifiable factors, including age, a family history of prostate cancer, and the levels of vitamin E, folic acid, and calcium in the body.
Yet there may be other lifestyle-related factors at play, and investigators are hard at work to uncover them.
Recently, a team of researchers from the University of Bristol and Imperial College London in the United Kingdom — alongside colleagues from other academic institutions across the globe — have used a different approach to try to find out more about prostate cancer risk factors.
In their new study, the findings of which now appear in the International Journal of Epidemiology, the investigators used a method called “Mendelian randomization.”
Mendelian randomization
allows researchers to look at genetic variations to assess causal relationships between various potential risk factors and the development of certain outcomes — in this case, prostate cancer.
Physical activity may more than halve risk
In their study, the researchers identified potential risk factors for prostate cancer through the World Cancer Research Fund’s (WCRF) 2018 systematic review of the evidence.
They also had access to the medical information of 79,148 participants with prostate cancer, as well as 61,106 participants without cancer who acted as the controls.
The analysis revealed that individuals with a genetic variation that increased their likelihood of being physically active had a 51% lower risk of prostate cancer than people who did not have this genetic variation.
Moreover, the researchers explain that “physical activity,” in this case, refers to all forms of activity, not just exercise.
Following on from this, the study authors conclude that interventions encouraging males to ramp up their levels of physical activity may have a protective effect against this widespread form of cancer.
“This study is the largest-ever of its kind, which uses a relatively new method that complements current observational research to discover what causes prostate cancer,” notes study co-author Sarah Lewis, Ph.D.
“It suggests that there could be a larger effect of physical activity on prostate cancer than previously thought, so will hopefully encourage men to be more active.”
Sarah Lewis, Ph.D.
Anna Diaz Font, who is head of research funding at WCRF — which, alongside Cancer Research U.K., funded this study — emphasizes the importance of the current findings.
“Up till now, there has only been limited evidence of an effect of physical activity on prostate cancer. This new study looked at the effect of 22 risk factors on prostate cancer, but the results for physical activity were the most striking,” she says.
The study’s findings, Diaz Font believes, “will pave the way for even more research, where similar methods could be applied to other lifestyle factors, to help identify ways men can reduce their risk of prostate cancer.”
https://moreliaclinic.com/wp-content/uploads/2015/08/FINAL-MORELIA-LOGO1.png00adminhttps://moreliaclinic.com/wp-content/uploads/2015/08/FINAL-MORELIA-LOGO1.pngadmin2019-12-09 20:44:262019-12-09 20:44:28New evidence suggests that being physically active could help slash prostate cancer risk.
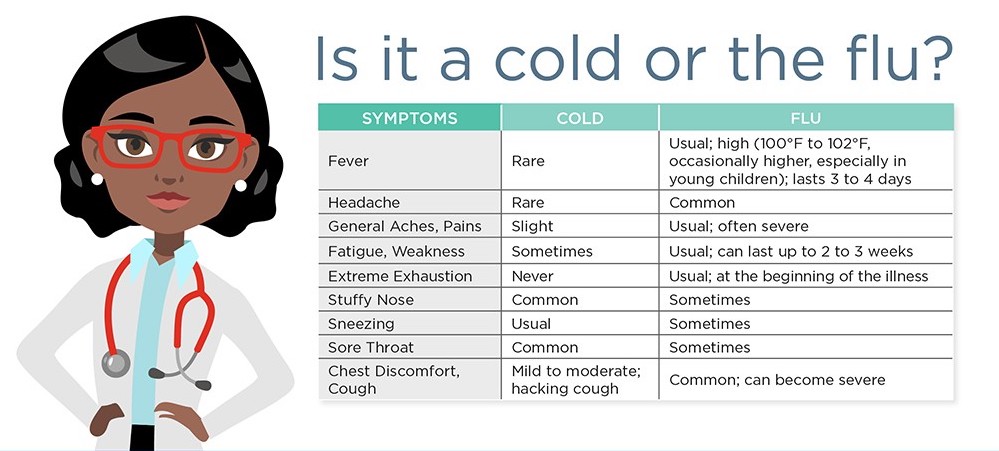
Both flu (influenza) and cold are caused by viruses, and they can have similar symptoms. So how do we know if a person has the flu or a bad cold? In this article, we explain the differences.
Cold and influenza are the most common illnesses in humans.
. Every year, 5-20 percent of the population of America develop flu symptoms.
The main difference between cold and flu is that, generally, symptoms of the flu are usually a lot more severe.
Each year, more than 200,000 people are hospitalized because of flu complications; flu is responsible for around 23,600 deaths every year.
Fast facts on colds vs. flu:
Colds and flu share many of the same symptoms; the major difference being flu is often worse, and accompanied by a high fever.
According to the Centers for Disease Control and Prevention (CDC), the average adult will have 2-3 colds every year.
The rhinovirus is the most common cause of cold.
The difference between cold and flu
Cold and flu are caused by different viruses, and, in general, the symptoms of flu are worse. Also, there are less likely to be serious complications from cold, such as pneumonia and bacterial infections.
The main difference between cold and flu symptoms is that flu more commonly includes fever; the fever can be 100 degrees Fahrenheit or higher and last for 3-5 days.
The extreme fatigue associated with flu can persist for weeks. Cold symptoms are generally milder and last about 1 week.
Also, runny nose or nasal congestion is more common with cold than flu.
Vomiting is another key difference; vomiting is not normally associated with the common cold but can be present in flu.
Although the differences above are generally true, without conducting special tests, it is impossible to know for sure whether it is flu or cold. For instance, it is possible to have flu without fever.
What is a cold?
Almost everybody is familiar with the sensation of having a cold. Colds affect both warm and cool climates equally, and the average person will have had many colds from infancy all the way until later life.
Symptoms include a runny nose, sore throat, coughing and sneezing, watery eyes, a headache, and body aches. There is no cure, except for resting and drinking plenty of fluids, but the cold should pass within 7-10 days.
There is normally no need to visit a doctor, but a person with a weakened immune system is more prone to developing pneumonia as a complication
To avoid catching or spreading a cold, people should wash their hands regularly and make sure they sneeze into a tissue or handkerchief, or into their elbow. This is the most hygienic as it stops the spread of germs, which cannot live on clothing or surfaces like they can on skin.
What is flu?
There are three types of flu virus, influenza A, influenza B, and influenza C. Types A and B are the ones that cause seasonal epidemics. One of the key symptoms of flu is feeling feverish or having a temperature of 100 degrees Fahrenheit or above. However, not everyone with the flu will have a fever.
Other symptoms include:
headaches or body aches
vomiting, nausea, and possibly diarrhea, especially in children
a sore throat and a cough
fatigue
chills and shivering
a congested or runny nose
A common cold is less likely to cause a high fever. With a cold, symptoms such as a runny nose or throat irritation will normally improve within a few days.
How to treat flu
The CDC note that the majority of people who have the flu do not need medical attention. Most can remain at home and avoid contact with other people to prevent the disease from spreading. However, the following treatments are available:
Over-the-counter medications – these can reduce fever. Tylenol can help people with flu feel more comfortable while they recover. Tylenol is also available to purchase online.
Prescription antiviral flu drugs – these are also available from a physician. They are for people who are at high risk of serious complications and are not normally necessary for effective treatment. They can only be given within a certain amount of time from symptom onset.
Home remedies – to alleviate symptoms, home remedies such as steam inhalation, nourishing foods like chicken soup, keeping warm, and other comfort measures can be used.
A physician will be able to decide if antivirals are needed. People who tend to be at greater risk include infants under the age of 2, people aged 65 years and older, and pregnant women.
Emergency warning signs for flu
Patients should seek medical help if they notice any of the emergency warning signs.
Warning signs in infants include difficulty breathing, having no appetite, and not producing tears when they cry, or having fewer wet diapers than usual.
Severe symptoms in older children include:
breathing problems
bluish skin color
not drinking enough fluids
not waking up or interacting
being so irritable that they do not want to be held
fever with a rash
If flu-like symptoms improve but then return with fever and a worse cough, the parent should consult a physician.
Anti-flu vaccines and other types of protection
The best way to protect against the flu is by having an annual vaccination, as this helps the body to build up the immune system so that it can fight off the virus more quickly.
The flu vaccine is recommended during pregnancy as it has been proven safe. If flu occurs during pregnancy, it can have serious complications for the unborn child and the mother.
https://moreliaclinic.com/wp-content/uploads/2015/08/FINAL-MORELIA-LOGO1.png00adminhttps://moreliaclinic.com/wp-content/uploads/2015/08/FINAL-MORELIA-LOGO1.pngadmin2019-12-02 19:51:462019-12-02 19:51:48What is the difference between cold and flu?
Vulvodynia and vestibulodynia refer to a chronic discomfort of the vulva, the part of a woman’s body that protects the genitals.
It includes the external female genitalia, including the mons pubis, the labia majora and minora, the clitoris, and the perineum.
Vulval pain can happen for a number of reasons, but vulvodynia and vestibulodynia are specifically linked to a hypersensitivity of the nerve endings in the skin.
Around 16 percent of women are estimated to have experienced pain or stinging in the vulval area at some time in their life.
Treatment
Treatment aims to alleviate symptoms. As the cause is unknown, finding a solution that works may take some trial and error.
Medications to block pain may include antidepressants, anticonvulsants, or serotonin-norepinephrine reuptake inhibitors (SNRIs).
Other solutions include creams, lotions, and anesthetic gel for applying to the vulval area.
Examples include topical hormone creams containing estrogen and testosterone, topical anesthetics, such as lidocaine, and products that contain an antidepressant or anticonvulsant ingredient. These can be applied 15 to 20 minutes before sexual activity, or when needed. Some of these products are available for purchase online, including lidocaine.
A nerve block is an anesthetic drug that is injected into the nerves that transmit pain signals, in this case, from the vulva to the spine. Interrupting the pain signals in this way can provide short-term relief.
If no other method is effective, surgery to remove the painful tissue may be appropriate.
Two techniques that are currently being investigated are neurostimulation and the spinal infusion pump.
Neurostimulation involves delivering low-voltage electrical stimulation to a specific nerve. This can replace pain with a tingling sensation.
A spinal infusion pump is an implanted device that can deliver low-dose medication to the spinal cord and nerve roots. This can dull pain.
However, there is limited evidence regarding the use of these measures for vulvodynia.
Some researchers have found that physical and psychosexual therapy can help improve sexual functioning, for example, by helping to reverse a fear of touch.
Symptoms
Vulvodynia features a burning, stinging, itching, irritating, or a raw feeling in the vulvar tissue, which may or may not appear inflamed. Patients may describe a feeling of throbbing, itching, aching, soreness, and swelling.
The pain can affect a particular spot, or it may be felt in a wider area, including the clitoris, the perineum, the mons pubis, and the inner thighs. It can also affect the area around the urethra and the top of the legs and inner thighs.
The pain involved in vulvodynia is neuropathic, which means it stems from abnormal signals from the nerve fibers in the vulval area. The nerve endings are hypersensitive.
It may be constant or intermittent. A constant pain that happens when there is no touch or pressure is known as unprovoked vulvodynia.
Vestibulodynia, previously known as vestibulitis, involves a pain that is triggered by light touch, or provoked pain.
Symptoms may be worse during or after sexual intercourse, walking, sitting, or exercising. It can happen when inserting a tampon, or when prolonged pressure is applied, for example, during horseback riding.
Vulvodynia is usually defined as lasting for at least 3 months. It often starts suddenly, and it may last for months or years. It is not life-threatening, but the pain can prevent the individual from carrying out some normal activities. This can also lead to upset or depression.
Complications
Relationship problems can result, because sexual intercourse is painful. One study suggests that 60 percent of women with vulvodynia are unable to engage in sex.
Studies suggest
that women who have vulvodynia can have a normal pregnancy, and that in some cases, pain levels fall during pregnancy. However, women with the condition are more likely to have a cesarean delivery.
Home remedies
Some measures can be taken that do not involve medications.
If vulvodynia occurs, the first step is to stop using any irritants, such as perfumed soaps. A change in menstrual products might help, for example, switching from synthetic to cotton-based items.
Cool gel packs may offer immediate, short-term pain relief. A range of cool gel packs is available for purchase online.
Pelvic floor muscle exercises may help by relaxing tissues in the pelvic floor and releasing tension in muscles and joints.
Biofeedback uses technology to increase an individual’s awareness of how they might be stressing their body. This information can help people change habits that lead to harm or discomfort. For women with vulvodynia, it can help strengthen the pelvic floor muscles, and this may reduce pain.
A trigger point is a specific area of discomfort. Trigger-point therapy involves massaging a small area of tightly contracted muscle to release tension and relieve pain. An anesthetic medication applied directly, for example, as a cream, can also be used to relieve pain in a trigger point.
Since stress can play a role in vulvodynia, either as a trigger or a consequence, stress management may help ease symptoms.
Acupuncture and cognitive behavior therapy are options currently being explored.
Diet
A change in diet may help. Cutting out one food at a time may help to pinpoint a trigger.
Items that commonly trigger a reaction include:
caffeine
high-sugar foods
acidic foods
processed foods
Causes
Vulvar pain can be caused by infections, neurological problems, inflammatory conditions, and neoplasms, such as squamous cell carcinoma.
Vulvodynia is not related to an underlying condition. The exact cause is unknown. It is not caused by a sexually transmitted or other infection, skin disease, or cancer, although these can also cause pain.
Factors that may raise the risk of vulvodynia include:
Damage to or irritation of the nerves around the vulva
A high density of pain-sensing nerve fibers in the vulval area
High levels of inflammatory substances in the vulval area, for example, because of inflammation
genetic susceptibility
pelvic floor muscles are weak or unstable
unusual or long-term reaction to infection, trauma, or another environmental factor
changes triggered by hormones
Other factors that increase susceptibility include:
frequent yeast infections
sexually transmitted infections (STIs)
chemical irritation of the external genitals, caused by soaps, feminine hygiene products or detergents in clothing
rashes on the genital area
previous laser treatments or surgery on the external genitals
nerve irritation, injury or muscle spasms in the pelvic area
diabetes
precancerous or cancerous conditions on the cervix
Provoked vestibulodynia could result from:
sexual intercourse
tampon insertion
a gynecologic examination
prolonged sitting
wearing tight underclothes or pants
activities such as cycling or horseback riding
Clitorodynia refers to pain in the clitoris.
Vulvodynia can be confused with other vulvovaginal problems, such as chronic tension or spasm of the muscles of the vulvar area called vaginismus.
Prevention
Measures that can reduce the risk of triggering pain include:
wearing cotton underwear and loose-fitting clothes around the genital area
avoiding scented toilet paper and perfumed creams and soaps
avoiding friction or sitting for prolonged periods
refraining from excessive genital washing
not douching or using vaginal wipes
using water-soluble lubricants during sexual intercourse
patting the area dry after rinsing or urinating
If a vaginal infection is suspected, it is important to have it diagnosed and treated promptly and to discuss with a physician if any treatments appear to make the condition worse.
Diagnosis
Diagnosis may involve a pelvic exam, to look for skin changes and assess the pain.
A cotton swab test is used to delineate the areas of pain and categorize their severity. The physician may press with swab on different areas while asking the patient to rate the level of pain.
The patient should be ready to describe the pain, including the type of pain and its severity, say when it started, and whether it began gradually or suddenly, where it hurts, and how often.
The doctor may use a special magnifying glass, to carry out a colposcopy.
Tests may be carried out to try to find the source of the pain and to eliminate other causes.
These include:
taking a culture for bacteria and yeast
blood tests to assess levels of estrogen, progesterone, and testosterone
a biopsy
In a biopsy, the doctor first numbs the genital area with a painkiller, and then a small piece of tissue is taken for examination under a microscope.
https://moreliaclinic.com/wp-content/uploads/2015/08/FINAL-MORELIA-LOGO1.png00adminhttps://moreliaclinic.com/wp-content/uploads/2015/08/FINAL-MORELIA-LOGO1.pngadmin2019-11-25 19:45:132019-11-25 19:45:16Vulvodynia: What you need to know
Insomnia is a sleep disorder that regularly affects millions of people worldwide. In short, individuals with insomnia find it difficult to fall asleep or stay asleep. The effects can be devastating.
Insomnia commonly leads to daytime sleepiness, lethargy, and a general feeling of being unwell, both mentally and physically. Mood swings, irritability, and anxiety are common associated symptoms.
Insomnia has also been associated with a higher risk of developing chronic diseases. According to the National Sleep Foundation, 30-40 percent of American adults report that they have had symptoms of insomnia within the last 12 months, and 10-15 percent of adults claim to have chronic insomnia.
Here, we will discuss what insomnia is, its causes, symptoms, diagnosis, and possible treatments.
Fast facts on insomnia:
There are many possible causes of insomnia.
An estimated 30-40 percent of Americans report experiencing insomnia each year.
Often, insomnia is due to a secondary cause, such as illness or lifestyle.
Causes of insomnia include psychological factors, medications, and hormone levels.
Treatments for insomnia can be medical or behavioral.
Causes
Insomnia can be caused by physical and psychological factors. There is sometimes an underlying medical condition that causes chronic insomnia, while transient insomnia may be due to a recent event or occurrence. Insomnia is commonly caused by:
Disruptions in circadian rhythm – jet lag, job shift changes, high altitudes, environmental noise, extreme heat or cold.
Hormones – estrogen, hormone shifts during menstruation.
Other factors – sleeping next to a snoring partner, parasites, genetic conditions, overactive mind, pregnancy.
Media technology in the bedroom
Several small studies in adults and children have suggested that an exposure to light from televisions and smartphones prior to going to sleep can affect natural melatonin levels and lead to increased time to sleep.
In addition, a study conducted by Rensselaer Polytechnic Institute found that backlit tablet computers can affect sleep patterns. These studies suggest that technology in the bedroom can worsen insomnia, leading to more complications.
Medications
According to the American Association of Retired Persons (AARP), the following medications can cause insomnia in some patients:
corticosteroids
statins
alpha blockers
beta blockers
SSRI antidepressants
ACE inhibitors
ARBs (angiotensin II-receptor blockers)
cholinesterase inhibitors
second generation (non-sedating) H1 agonists
glucosamine/chondroitin
Signs and symptoms
Insomnia itself may be a symptom of an underlying medical condition. However, there are many signs and symptoms that are associated with insomnia:
Difficulty falling asleep at night.
Waking during the night.
Waking earlier than desired.
Still feeling tired after a night’s sleep.
Daytime fatigue or sleepiness.
Irritability, depression, or anxiety.
Poor concentration and focus.
Being uncoordinated, an increase in errors or accidents.
Tension headaches (feels like a tight band around head).
Difficulty socializing.
Gastrointestinal symptoms.
Worrying about sleeping.
Sleep deprivation can cause other symptoms. The afflicted person may wake up not feeling fully awake and refreshed, and may have a sensation of tiredness and sleepiness throughout the day.
Having problems concentrating and focusing on tasks is common for people with insomnia. According to the National Heart, Lung, and Blood Institute, 20 percent
Types
Insomnia includes a wide range of sleeping disorders, from lack of sleep quality to lack of sleep quantity. Insomnia is commonly separated into three types:
Transient insomnia – occurs when symptoms last up to three nights.
Acute insomnia – also called short-term insomnia. Symptoms persist for several weeks.
Chronic insomnia – this type lasts for months, and sometimes years. According to the National Institutes of HealthTrusted Source
, the majority of chronic insomnia cases are side effects resulting from another primary problem.
Treatment
Good sleep hygiene, including avoiding electronics before bed, can help treat insomnia.
Some types of insomnia resolve when the underlying cause is treated or wears off. In general, insomnia treatment focuses on determining the cause.
Once identified, this underlying cause can be properly treated or corrected.
In addition to treating the underlying cause of insomnia, both medical and non-pharmacological (behavioral) treatments may be used as therapies.
Non-pharmacological approaches include cognitive behaviorlal therapy (CBT) in one-on-one counseling sessions or group therapy:
Medical treatments for insomnia include:
prescription sleeping pills
antidepressants
sleep aids available online or over-the-counter
antihistamines
melatonin, which can be purchased online
ramelteon
Home remedies
Home remedies for insomnia include:
Improving “sleep hygiene”: Not sleeping too much or too little, exercising daily, not forcing sleep, maintaining a regular sleep schedule, avoiding caffeine at night, avoiding smoking, avoiding going to bed hungry, and ensuring a comfortable sleeping environment.
Using relaxation techniques: Examples include meditation and muscle relaxation.
Stimulus control therapy – only go to bed when sleepy. Avoid watching TV, reading, eating, or worrying in bed. Set an alarm for the same time every morning (even weekends) and avoid long daytime naps.
Sleep restriction: Decreasing the time spent in bed and partially depriving the body of sleep can increase tiredness, ready for the next night.
Diagnosis
A sleep specialist will start by asking questions about the individual’s medical history and sleep patterns.
A physical exam may be conducted to look for possible underlying conditions. The doctor might screen for psychiatric disorders and drug and alcohol use.
The Stanford Center for Sleep Sciences and Medicine explains that the term “insomnia” is often used to refer to “disturbed sleep.”
For a diagnosis of insomnia, the disturbed sleep should have lasted for more than 1 month. It should also negatively impact the patient’s wellbeing, either through the causing distress or disturbing mood or performance.
The patient may be asked to keep a sleep diary to help understand their sleeping patterns.
Other tests may include a polysomnograph. This is an overnight sleeping test that records sleep patterns. In addition, actigraphy may be conducted. This uses a small, wrist-worn device called an actigraph to measure movement and sleep-wake patterns.
Risk factors
Insomnia can affect people of any age; it is more common in adult females
than adult males. It can undermine school and work performance, as well as contributing to obesity, anxiety, depression, irritability, concentration problems, memory problems, poor immune system function, and reduced reaction time.
Some people are more likely to experience insomnia. These include:
travelers, particularly through multiple time zones
shift workers with frequent changes in shifts (day vs. night)
the elderly
users of illegal drugs
adolescent or young adult students
pregnant women
menopausal women
those with mental health disorders
https://moreliaclinic.com/wp-content/uploads/2015/08/FINAL-MORELIA-LOGO1.png00adminhttps://moreliaclinic.com/wp-content/uploads/2015/08/FINAL-MORELIA-LOGO1.pngadmin2019-11-18 20:26:212019-11-18 20:26:24Insomnia: Everything you need to know
The flu is a common respiratory infection, and its symptoms can range from mild to severe. Although a rash is not a common symptom of the flu, it can sometimes occur.
There is evidence to suggest that certain types of flu may lead to a rash forming in some people. In other cases, another condition may cause a rash to develop when a person has the flu.
In this article, learn more about a flu rash, including the symptoms, diagnosis, and treatment.
Can the flu cause a rash?
The flu causes many uncomfortable symptoms, but a rash is typically not one of them. There is some evidence, however, that the flu may sometimes cause a rash.
A small 2014 case study
of school-aged children found that a rash is a possible symptom of influenza type B.
The authors indicated that other factors, aside from the flu, might have contributed to the onset of the rash, such as a measles outbreak in a nearby area.
The authors of an older article
from 2011 stated that a rash occurs in about 2% of all influenza A cases. The researchers indicated that the rash could occur among children with or without accompanying viral or bacterial infections or environmental factors.
Other symptoms
The flu has several recognizable symptoms that a person will typically experience during the infection.
In most cases, the flu will clear on its own within a few days to 2 weeks
According to the Centers for Disease Control and Prevention (CDC)
, the typical symptoms of the flu include:
a cough
chills
a fever
body aches
a sore throat
fatigue
a stuffy or runny nose
headaches
vomiting or diarrhea
In some cases, a person may develop health complications as a result of the flu. Some of these, such as pneumonia, can be life threatening.
Other complications may include:
worsened asthma symptoms
swelling of heart, brain, or muscle tissues
heart or kidney failure
extreme inflammatory responses in the body
Other causes of a rash
Certain other viruses could potentially cause a rash. Some of these viruses may have symptoms similar to those of the flu and be easy to mistake for this illness at first.
For example, a person may develop flu-like symptoms prior to developing a measles rash.
Some common measles symptoms that may appear before the rash occurs include:
a runny nose
a fever
fatigue
a cough
body aches and pains
Some other common viral infections that may cause a rash include:
chickenpox
rubella
fifth disease
roseola
West Nile virus
dengue fever
hand, foot, and mouth disease
mononucleosis
Zika virus
In some cases, another condition may cause a rash in someone who already has the flu.
Diagnosis
If flu-like symptoms occur alongside a rash, it is best to speak to a doctor. During the appointment, the doctor will conduct a physical examination and ask about the person’s symptoms.
During times when the flu is widespread, the doctor may not need to test for the virus. However, when this is not the case, the doctor may test for the type of virus.
A doctor can also examine the rash and determine whether it may be due to a different condition.
Treatment
If a person has the flu, the typical treatment involves extra rest and fluids. However, people with severe infections and those at risk of developing complications may receive antiviral medications from a doctor.
These medications can help the person recover from their flu more quickly and prevent further complications. Some examples include:
peramivir (Rapivab)
oseltamivir (Tamiflu)
baloxavir (Xofluza)
zanamivir (Relenza)
If a person has the flu and a rash, a doctor may not treat the rash directly. Instead, the rash should clear when the body fights off the virus.
3 Foods Dogs Shouldn’t Eat
What’s missing in most dog food? Get this top US vet’s dog food topper to help
longevity. – NutraThrive
When to see a doctor
Anyone can develop the flu, even otherwise healthy individuals. However, certain groups of people have a higher risk of developing complications. These individuals include:
older people
children under the age of 5 years
pregnant women
people with chronic illnesses, such as asthma, diabetes, or heart disease
Although most cases of the flu will resolve with plenty of rest and fluids, people who are at risk of complications should see a doctor.
In some cases, a person may need to seek immediate medical attention. People with the flu should seek emergency medical care if they experience any of the following:
persistent pain or pressure in the chest or abdomen
difficulty breathing
seizures
severe muscle pain
shortness of breath
a fever or cough that improves but then returns or worsens
persistent confusion or dizziness
worsening of chronic medical conditions
lack of urination
severe weakness or unsteadiness
Parents or caregivers should seek emergency care
for a child who has:
bluish lips or face
severe muscle pain
fast breathing or trouble breathing
seizures
ribs pulling in with each breath
chest pain
a fever or cough that improves before returning or worsening
dehydration, signs of which can include little urine, no tears, and a dry mouth
a lack of alertness
the inability to interact when awake
a fever above 104°F or any fever in infants under 12 weeks old
worsening symptoms of chronic medical conditions
Summary
A rash is a possible but uncommon symptom of the flu. If a rash appears due to the flu or another virus, it should clear when the virus is no longer active.
A person should see their doctor if they have an unexplained rash or severe flu symptoms. A doctor can also help determine whether the rash is due to the flu or another condition.
https://moreliaclinic.com/wp-content/uploads/2015/08/FINAL-MORELIA-LOGO1.png00adminhttps://moreliaclinic.com/wp-content/uploads/2015/08/FINAL-MORELIA-LOGO1.pngadmin2019-11-11 21:16:332019-11-11 21:16:36Flu rash: Everything you need to know
Rare diseases are by their very nature obscure and unknown, falling through the cracks when it comes to research budgets and treatment development. But now, a study has shown they are more common than we think.
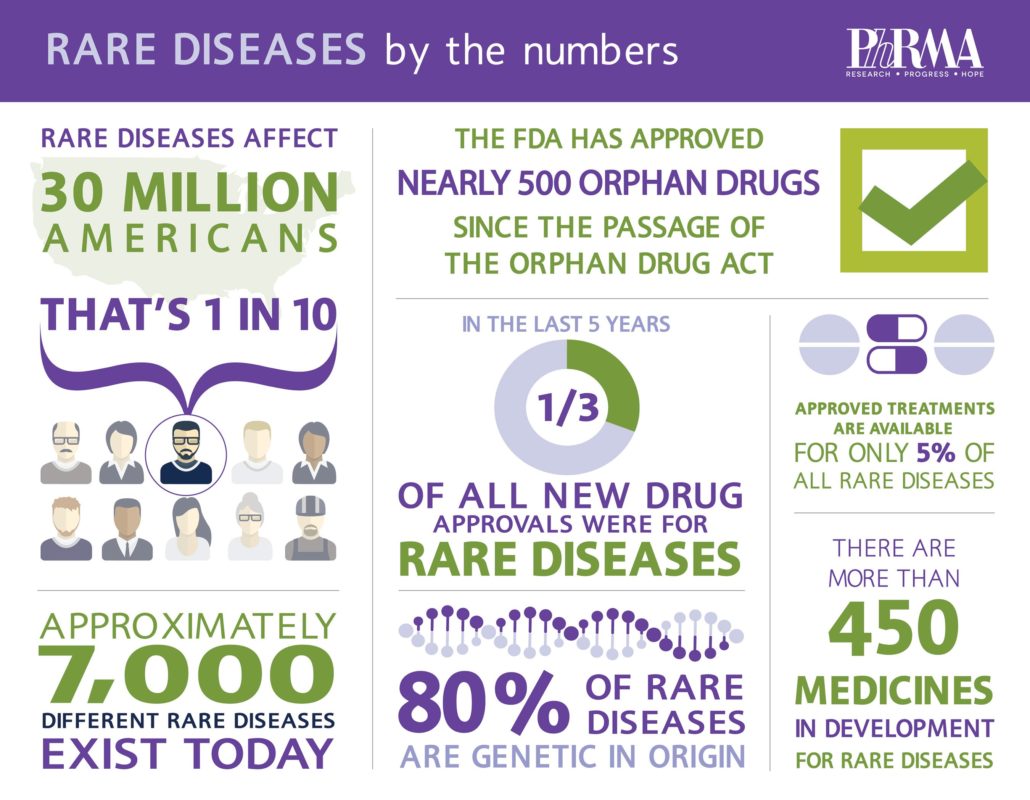
The United States classifies a rare disease as one that affects fewer than 200,000 people. However, all together, rare diseases in the U.S. affect 25–30 million people.
While the diseases themselves may be rare, this significant figure highlights just how many people are living with diseases that get little attention due to their singularity.
Until the recent study, scientists had no real concept of the prevalence of rare diseases globally.
The few studies into the incidence of rare diseases have seldom looked at population registries, making it hard to establish prevalence with precision.
As in the U.S., most countries do not track rare diseases. In fact, they document very few even after diagnosis. This makes it tricky to work out the exact number of rare diseases or how many people are living with them.
Now an analysis of the Orphanet database, which is a comprehensive record of the incidence of rare disease, indicates that over 300 million people globally are living with a rare disease.
‘A low estimation of the reality’
“In all likelihood, our data represent a low estimation of the reality. The majority of rare diseases are not traceable in healthcare systems, and in many countries, there are no national registries,” says Ana Rath, the director of Inserm US14 in Paris, France.
The National Institute for Health and Medical Research (INSERM) in France established Orphanet in 1997 to improve knowledge of rare diseases and boost awareness, diagnosis, and treatment of people living with them.
Today, a consortium of 40 countries work together to pool data on rare diseases, making it the most comprehensive source of data on the topic.
Researchers hope that by highlighting the number of individuals impacted by a rare disease and showing that rare disease is “not so rare,” public health policies at a national and global level will begin to address the issue.
“Given that little is known about rare diseases, we could be forgiven for thinking that [those living with them] are thin on the ground,” says Rath. “But when taken together, they represent a large proportion of the population.”
According to the Genetic and Rare Diseases Information Center (GARD), there may be as many as 7,000 rare diseases. Experts often refer to these diseases as orphan diseases because drug companies have tended to neglect them by excluding them from their drug research and treatment development budgets.
, which passed in the U.S. in 1983, offered pharmaceutical companies a financial incentive to develop drugs for rare diseases, such as polycythemia vera, Marfan syndrome, and systemic sclerosis.
However, there is still no available treatment for most rare diseases.
Many scientists have serious concerns about the impact that these rare diseases have on those living with them and their families around the world.
4% of the population have a rare disease
The researchers did not include some cancers or other rare conditions induced by infection or poisoning in their investigation. However, they analyzed 3,585 rare diseases to find out how many people globally have the disease at the same time. The results showed that 3.5–5.9% of the world’s population have these conditions at any given time.
The study also found that 80% of those with a rare disease had one of only 149 illnesses.
In addition, 71.9% of the diseases on Orphanet had genetic causes, and 69.9% began in childhood.
The research concludes that rare diseases are not so rare, after all.
In the study abstract, the authors refer to rare diseases as “an emerging global public health priority.”
The researchers call for the findings to shine a light on research priorities, emphasize the societal impact of these conditions, and highlight the need for a comprehensive public health policy, both on a national and global level.
The focus going forward is on examining those diseases not included in the study and building knowledge on rare diseases to ensure that people receive better care.
“Making patients visible within their respective healthcare systems by implementing means to record their precise diagnoses would make it possible in the future not only to review our estimations but more fundamentally to improve the adaptation of support and reimbursement policies.”
Ana Rath
In the U.S., the Office of Orphan Products Development (OOPD)
runs a program to incentivize drug companies to develop treatments for rare diseases. The 10 years between 1973 and 1983 saw the approval of just 10 treatments for rare diseases. But since then, the OOPD have overseen the development of more than 400 drugs and products.
https://moreliaclinic.com/wp-content/uploads/2015/08/FINAL-MORELIA-LOGO1.png00adminhttps://moreliaclinic.com/wp-content/uploads/2015/08/FINAL-MORELIA-LOGO1.pngadmin2019-11-07 21:37:032019-11-07 21:37:06Rare diseases more common than we think
Type 1 diabetes has no cure, and although there are several treatment options available, many people find managing the condition challenging. New technology could help reduce that burden.
Many people find managing type 1 diabetes inconvenient, but new research may change this.
More than 1 million children and adults in the United States have type 1 diabetes, according to the American Diabetes Association.
The Centers for Disease Control and Prevention (CDC) note that about 5%
Trusted Source
of all people who have diabetes have type 1.
Type 1 diabetes can significantly impact a person’s life, as people need to monitor their blood sugar levels regularly to ensure they do not become dangerously high or low.
Currently, people with type 1 diabetes measure their blood sugar levels by pricking a finger several times a day or wearing a glucose monitor. Depending on the measurements, they may have to administer insulin using an injection or insulin pump.
But a new form of technology trialed recently and showcased in the New England Journal of Medicine could replace these conventional methods.
Automatic insulin
The trial looked at a particular type of artificial pancreas, or closed-loop control. These devices continuously monitor and regulate blood glucose levels. When the monitor detects that a person needs insulin, a pump releases the hormone into the body.
The trial involved the use of the Control-IQ system — a new type of artificial pancreas that uses algorithms to adjust insulin doses automatically throughout the day.
“By making management of type 1 diabetes easier and more precise, this technology could reduce the daily burden of this disease, while also potentially reducing diabetes complications, including eye, nerve, and kidney diseases,” says Dr. Griffin P. Rodgers, director of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK).
The 6-month trial is part of a much larger research initiative known as the International Diabetes Closed-Loop (iDCL) Study, which involves the testing of several artificial pancreas systems to determine a variety of factors, such as safety, effectiveness, and user-friendliness.
The trial recruited 168 people with type 1 diabetes and with a minimum age of 14.
The researchers assigned over 100 people to use the Control-IQ system, while 56 people formed a control group that used sensor-augmented pump (SAP) therapy. This therapy does not alter insulin doses automatically.
Researchers wanted to replicate day-to-day life, so they did not monitor the systems remotely. Participants did, however, contact researchers every few weeks to check data from the device.
24-hour control
The researchers were interested in the amount of time that blood glucose levels reached a target range of 70 to 180 milligrams per deciliter (mg/dl).
The results showed that the blood sugar levels of the people who used the Control-IQ system were in the target range for an average of 2.6 hours per day longer than previously. Those using the SAP therapy saw no notable change throughout the trial.
Vitally, the system also improved the participants’ blood glucose control overnight as well as during the day. This is a crucial advancement for people whose levels drop significantly when asleep.
None of the groups experienced severe cases of hypoglycemia — when blood sugar levels become very low.
Reducing the burden
According to Dr. Guillermo Arreaza-Rubín, the study’s program scientist and director of NIDDK’s Diabetes Technology Program, these findings indicate that this system “has the potential to improve the health of people living with type 1 diabetes, while also potentially lifting much of the burden of care from those with the disease and their caregivers.”
Boris Kovatchev, Ph.D., director of the UVA Center for Diabetes Technology, says the technology’s glucose control is “beyond what is achievable using traditional methods.”
The team has submitted the results of the trial to the U.S. Food and Drug Administration (FDA). They are waiting to find out whether the device can go to market.
https://moreliaclinic.com/wp-content/uploads/2015/08/FINAL-MORELIA-LOGO1.png00adminhttps://moreliaclinic.com/wp-content/uploads/2015/08/FINAL-MORELIA-LOGO1.pngadmin2019-10-28 20:20:052019-10-28 20:20:07New technology better controls type 1 diabetes
New research finds that the placebo effect may be socially contagious. In other words, a doctor’s beliefs about whether or not a pain treatment will work can exert a subtle influence on how much pain the patient will actually experience.
A doctor’s display of confidence in a treatment may make it more effective.
The power of placebo may extend beyond what researchers previously believed.
At first, they only used placebos as controls in drug experiments.
With time, however, placebos proved to have value as potential treatments in their own right.
Pain, depression, anxiety, irritable bowel syndrome, Parkinson’s disease, and epilepsy are only some of the conditions that placebos have shown promise in treating.
A new study has looked into another fascinating aspect of the placebo: Does it transmit socially, from one person to another? If so, how? More specifically, how does a doctor’s belief about the effects of a medication affect their patient’s experience of pain?
Laboratory at Dartmouth College in Hanover, NH — is the corresponding author of the new study.
Chang and colleagues have published their findings in the journal Nature Human Behaviour
Testing placebo power in 3 experiments
To study the phenomenon of socially transmitted placebo, the researchers devised three experiments. All three involved two different creams that were meant to relieve heat-induced pain by targeting pain receptors on the participants’ skin.
One of the creams was called thermedol, and the other was a control cream. Although different in appearance, both creams were actually placebos — namely, petroleum jelly with no pain relieving properties at all.
The researchers asked undergraduate students to play the roles of “doctors” and “patients.” They informed the “doctors” of the creams’ benefits and conditioned them to believe that thermedol was better at relieving pain than the control cream.
The first experiment consisted of 24 “doctor-patient” pairs. In each pair, the “patient” did not know which cream was thermedol and which was the control. Only the “doctor” knew which was the “effective” cream.
The researchers then applied the creams to the participants’ arms, followed by pain-inducing heat, in order to evaluate the effects of the cream. All participants received the same amount of heat.
During the experiment, all participants wore cameras that recorded their facial expressions in the doctor-patient interactions.
Using a machine-learning algorithm trained on facial signals of pain, the researchers were able to examine the effect of cues such as raised eyebrows, raised upper lips, or nose wrinkling on the perceived effectiveness of the treatments.
In this experiment, the participants reported experiencing less pain with thermedol, and skin conductance tests suggested that they actually did experience less discomfort. Their facial expressions also reflected less pain with thermedol.
In the other two experiments, the researchers applied the creams in different orders, and they led the doctors to believe that they were using thermedol when they were using the control creams, and vice versa.
The experimenters themselves were also blind to the study, not knowing which cream was which. In these experiments, the results were the same.
How doctors’ beliefs affect clinical results
Overall, across all three experiments, the results revealed that when the “doctors” believed that a treatment was effective, the “patients” reported feeling less pain. Their facial expressions and skin conductance tests also revealed fewer signs of pain.
The reasons for this remain unclear. However, the researchers believe that social contagion via facial cues is the most likely explanation.
“When the doctor thought that the treatment was going to work, the patient reported feeling that the doctor was more empathetic,” says Chang.
“The doctor may have come across as warmer or more attentive. Yet, we don’t know exactly what the doctor was doing differently to convey these beliefs that a treatment works. That’s the next thing that we’re going to explore,” he adds.
“What we do know though is that these expectations are not being conveyed verbally but through subtle social cues,” explains Chang.
“These findings demonstrate how subtle social interactions can impact clinical outcomes. You can imagine that in a real clinical context, if the healthcare providers seemed competent, empathetic, and confident that a treatment may work, the impact on patient outcomes could be even stronger.”
https://moreliaclinic.com/wp-content/uploads/2015/08/FINAL-MORELIA-LOGO1.png00adminhttps://moreliaclinic.com/wp-content/uploads/2015/08/FINAL-MORELIA-LOGO1.pngadmin2019-10-23 21:44:352019-10-23 21:44:37Doctors’ beliefs about treatment affect patients’ experience of pain
Researchers believe that stress and cardiovascular health are linked in some way, but the association is not yet fully clear. A large-scale new study has recently delved into the effects of a unique kind of stress.
According to the American Heart Association (AHA), stress may affect factors that increase the risk of heart disease, including blood pressure and cholesterol level.
One major source of stress is the workplace.
In fact, a 2015 review of 27 studies that appeared in the journal Current Cardiology Reports
found an association between work stress and a “moderately elevated risk of incident coronary heart disease and stroke.”
However, one type of stress that researchers often leave out of studies is that felt by a person who needs to simultaneously balance the demands of work and family life.
Examining this in more depth may eventually help health professionals better identify and treat cardiovascular issues. This is according to the authors of the new study, which now appears in the Journal of the American Heart Association.
What is work-family conflict?
Cardiovascular diseases are currently the leading cause of death worldwide, say the World Health Organization (WHO).
Health professionals can determine people’s cardiovascular health score. Based on seven metrics including diet, blood pressure, and physical activity levels, the researchers who conducted the new study used this score to investigate how work and family stress can impact heart health.
According to the study paper, work-family conflict refers to “a form of inter-role conflict in which the role pressures from the work and family domains are mutually incompatible in some respect.”
More than 11,000 workers ages 35–74, from six state capitals in Brazil, made up the study’s sample. The participants came from a variety of educational and work backgrounds, and the study included a slightly higher number of women.
Each participant filled out a questionnaire to determine how their job affected their family life, and how their family life impacted their work.
The researchers calculated the participants’ cardiovascular health scores using a combination of clinical examinations, laboratory test results, and self-reported questionnaires.
An unequal impact
The analysis showed a distinct sex difference. Men reported less work interference with family and more time for personal care and leisure. Both sexes reported a similar amount of family interference with work.
However, women appeared to be worse off. Those who reported a number of frequent work-family conflicts had lower cardiovascular health scores.
“This was interesting because in our previous study, job stress alone affected men and women almost equally,” says senior study author Dr. Itamar Santos, a professor at the University of São Paulo in Brazil.
There could be a simple explanation as to why this is the case, and it has to do with traditional gender roles. “You feel the stress to fulfill the gender roles, and I think women still feel more of a need to have that nurturing home life,” says Dr. Gina Price Lundberg, clinical director of the Emory Women’s Heart Center in Atlanta, GA.
“Men are helping more than ever, but I think working women still feel the stress of trying to do it all.” She goes on to describe the study as “well-designed,” due to its large sample size, the diverse background of the participants, and the balance of men and women.
However, certain elements of the study relied on the participants’ own thoughts and feelings, which may have biased the results.
How to live with stress
What this study has dipped into is the need for a good work-life balance. However, this is easier said than done in many cases.
Dr. Santos hopes that the new findings will encourage workplaces to introduce stress reducing initiatives and encourage doctors to look for signs of stress when examining people.
“We’re not going to eliminate stress,” Dr. Santos says. “But we should learn how to live with it to not have so many bad consequences.”
Whether that would be through measures such as at-home meditation or employer-led strategies is yet to be determined.
Dr. Santos and team are now planning to follow the same participants for up to a decade to gain further insight.
https://moreliaclinic.com/wp-content/uploads/2015/08/FINAL-MORELIA-LOGO1.png00adminhttps://moreliaclinic.com/wp-content/uploads/2015/08/FINAL-MORELIA-LOGO1.pngadmin2019-10-21 20:46:542019-10-21 20:46:56Balancing work and family life puts a strain on women’s heart health.
New blood test detects brain tumors with 87% accuracy
Dr. Matthew J. Baker, a reader in the Department of Pure and Applied Chemistry at the University of Strathclyde in Glasgow, United Kingdom, is the lead author of the new research.
He and his colleagues have now published their findings in the journal Nature Communications.
Of the study, Dr. Baker says, “This is the first publication of data from our clinical feasibility study, and it is the first demonstration that our blood test works in the clinic.”
Although it is quite rare, brain cancer often has a poor outlook.
According to the National Cancer Institute, around 0.6% of people will develop brain cancer or another cancer of the nervous system in their lifetime.
However, the 5 year survival rate for those who do receive such a diagnosis is less than 33%.
Largely, the poor outlook is due to the fact that brain tumors have very nonspecific symptoms, which makes them more difficult to distinguish from other conditions.
Study co-author Dr. Paul Brennan — a senior clinical lecturer and consultant neurosurgeon at the University of Edinburgh in the U.K. — explains, “Diagnosing brain tumors is difficult, leading to delays and frustration for lots of people.”
“The problem is that symptoms of brain tumor are quite nonspecific, such as headache, or memory problems. It can be difficult for doctors to tell which people are most likely to have a brain tumor,” he adds.
The lack of cost effective tests that can help doctors triage people with brain tumors in primary care also means that it takes longer to accurately diagnose brain cancer. This ultimately results in a poorer outlook.
The team’s new blood test brings much needed hope in this regard. Dr. Baker and colleagues used infrared light to create a “bio-signature” of people’s blood samples and applied artificial intelligence to scan for signs of cancer.
The test correctly identified brain cancer in a cohort of 104 people 87% of the time.
A more rapid means of diagnosis
As the researchers explain in their paper, they used a technique called attenuated total reflection-Fourier transform infrared (ATR-FTIR) spectroscopy and coupled it with machine learning technology to detect brain cancer.
The authors explain that the technique is “a simple, label free, noninvasive, nondestructive” way of analyzing the biochemical profile of a blood sample without requiring extensive preparation of the sample.
The ATR-FTIR technique allowed the researchers to work out a biochemical “fingerprint” of brain cancer.
Dr. Baker and team trained a machine learning algorithm to use these biochemical fingerprints to diagnose brain cancer in a retrospective cohort of 724 people. This cohort included people with primary and secondary cancers as well as control participants without cancer.
They then used the algorithm to predict brain cancer cases in a sample of 104 participants. Of these, 12 people had cancer, including four cases of glioblastoma. This is one of the most aggressive forms of brain tumor.
The findings revealed a sensitivity of 83.3% and a specificity of 87% for the blood test. “With this new test, we have shown that we can help doctors quickly identify which [people] with these nonspecific symptoms should be prioritized for urgent brain imaging,” says Dr. Brennan.
“This,” he adds, “means a more rapid diagnosis for people with a brain tumor, and quicker access to treatment.”
Hayley Smith — an ambassador for the Brain Tumor Charity in Hampshire, U.K. — adds that it is “very encouraging to hear that this blood test can lead to a quicker diagnosis for brain cancer.”
“This kind of test will be vital to patients, helping people to get the correct diagnosis quicker, which ultimately will help people to get the urgent medical care that they need.”
https://moreliaclinic.com/wp-content/uploads/2015/08/FINAL-MORELIA-LOGO1.png00adminhttps://moreliaclinic.com/wp-content/uploads/2015/08/FINAL-MORELIA-LOGO1.pngadmin2019-10-18 18:50:572019-10-18 18:50:59A simple blood test could make a great difference for those with brain cancer.